


Lunchtime Pandemic Reading, 5-June-2020
Delayed, sorry about that

NB: This didn’t send on Friday. Sending this out now and today’s in a little bit.
—
Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
--
The final nail in the coffin for hydroxychloroquine and COVID-19. "Amajor clinical trial showed the malaria drug hydroxychloroquine had no benefit for patients hospitalized with Covid-19, likely closing the door to the use of the highly publicized medicine in the sickest patients — a use for which it was widely prescribed as the pandemic hit the U.S.
The results come from a study called RECOVERY, funded by the U.K. government, that sought to randomly assign large numbers of patients to multiple potential treatments in the country’s National Health Service. The goal was to rapidly get answers as to what worked and what didn’t.
“Today’s preliminary results from the RECOVERY trial are quite clear – hydroxychloroquine does not reduce the risk of death among hospitalized patients with this new disease,” University of Oxford epidemiologist Martin Landray, one of the study’s leaders, said in a statement. “This result should change medical practice worldwide and demonstrates the importance of large, randomized trials to inform decisions about both the efficacy and the safety of treatments.”"
Source: https://www.statnews.com/2020/06/05/hydroxychloroquine-had-no-benefit-for-hospitalized-covid-19-patients-possibly-closing-door-to-use-of-drug/
Commentary: At this point, we now have clinical data for every phase of COVID-19 that says hydroxychloroquine is of no value and substantial potential harm for treating COVID-19. Disbelieve anyone, especially politicians, who say otherwise.
--
CDC needs to remind people that pets should not wear masks or be subject to disinfectants. "It’s not safe to put a face covering on your pet or use disinfectants not meant for animals. The risk of animals spreading #COVID19 is considered to be low. Protect pets by limiting their contact w/ people & other animals outside the household. Learn more: https://bit.ly/2z9q5be"
Source:


Commentary: You know some poor pet was subject to injury from disinfectants. The reality is that pets are like infants and toddlers. You're not going to keep a mask on them anyway, and as long as you limit their contact with others, they'll be fine and unlikely to further the spread of the disease.
--
The international quest for a vaccine races ahead with 133 candidates and 10 in trials. "Wondering where things stand with development of #Covid19 vaccines? @WHO's latest update shows 133 vaccines are in development, 10 already in human trials. Many of these won't make it thru the pipeline, but this is still rather amazing."
Source:

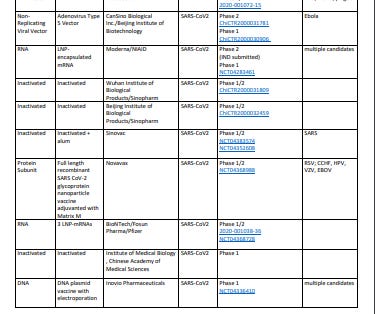
Source: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines
Commentary: This bodes well for the development of a vaccine, that so many candidates are in the pipeline. Let's hope we get some working ones that pass all four phases of the clinical trial process, but as Stat News said, this is amazing for a disease we didn't know about 7 months ago and speaks well of the scientific community as a whole.
--
Asymptomatic people with COVID-19 appear to clear it faster, owing to lower viral loads, but are still contagious. "Between March 10th and April 4th, 2020, 14,000 quarantined people were tested for SARS-CoV-2; 49 were positive. Of these, 30 participated in the study: 13(43%) never had symptoms and 17(57%) were symptomatic. 17(57%) participants acquired their infection outside Vietnam. Compared with symptomatic individuals, asymptomatic people were less likely to have detectable SARS-CoV-2 in NTS samples collected at enrolment (8/13 (62%) vs. 17/17 (100%) P=0.02). SARS-CoV-2 RNA was detected in 20/27 (74%) available saliva; 7/11 (64%) in the asymptomatic and 13/16 (81%) in the symptomatic group (P=0.56). Analysis of the probability of RT-PCR positivity showed asymptomatic participants had faster viral clearance than symptomatic participants (P<0.001 for difference over first 19 days). This difference was most pronounced during the first week of follow-up. Two of the asymptomatic individuals appeared to transmit the infection to up to four contacts. Asymptomatic SARS-CoV-2 infection is common and can be detected by analysis of saliva or NTS. NTS viral loads fall faster in asymptomatic individuals, but they appear able to transmit the virus to others."
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa711/5851471#.Xtm1o5p1gxV.twitter
Commentary: Asymptomatic does not mean non-contagious. This is important to remember. Masks on, everywhere outside your home but especially indoors. (stores, etc.)
--
A thoughtful piece by the AMA Journal of Ethics going into the weekend: social justice is part of public health, and doctors should consider participating. "Classifying mortality by root social causes illustrates the importance of a public health approach to medical care. For instance, in 2000, there were 193,000 deaths attributed to acute myocardial infarction, 168,000 to cerebrovascular disease, and 156,000 to lung cancer. But when one group of researchers examined the actual contributing causes, they ended up with very different results: they found that 245,000 deaths were attributable to low education, 162,000 to racial segregation, 162,000 to low social support, 133,000 to individual-level poverty, and 119,000 to income inequality [13].
A few studies show how effective changes in social policy could lead to changes in health outcomes. One group calculated that equalizing the mortality rates of whites and African-Americans would have averted 686,202 deaths between 1991 and 2000, whereas medical advances over the same period averted only 176,633 deaths [14]. Another calculated that 880,000 deaths per year would be averted in the US if the country had a smaller income gap, like those of many Western European nations, and their stronger social safety nets [15].
It’s preventive medicine writ large: injustice, oppression, war, environmental damage—all affect our patients. As professionals dedicated to healing and health, physicians should advocate on behalf of the vulnerable and disenfranchised (including the poor, racial and ethnic minorities, lesbian/gay/bisexual/transgender people, children, the disabled, HIV-infected patients, those with mental illness, undocumented immigrants, the homeless, victims of violence, and prisoners), whose voices are often unheard and whose oppression has medical consequences."
Source: https://journalofethics.ama-assn.org/article/call-service-social-justice-public-health-issue/2014-09
Commentary: It's worthwhile noting that many people, in the early days of the pandemic, cited flu figures and said, "the flu is worse, no need to protect ourselves from the pandemic" but not a single one said "racism is worse", yet in a single year, racism killed more people than COVID-19 has thus far, by several times. We are seeing clear disparities in health outcomes based on race and socioeconomic background. If we want to minimize loss of life through this and future public health emergencies, we also need to solve the underlying systemic problems that make it easier for pandemics to injure or kill the disadvantaged.
--
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are never to be ingested.
2. Wear gloves and a mask when out of your home. Consider wearing a face shield.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters. Avoid indoor places as much as you can.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Donate any PPE you can. https://getusppe.org/give/
--
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
--
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.