


Lunchtime Pandemic Reading, 28-January-2022
Happy 2 year anniversary?

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from a qualified healthcare provider who knows your specific medical situation over advice from people on the Internet.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
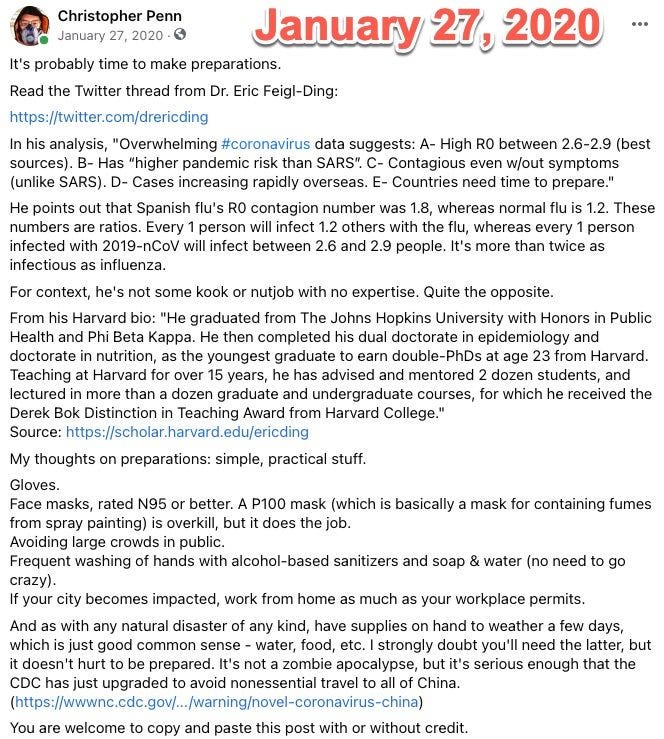
This is the second anniversary of this newsletter, which first started as Facebook posts on January 27, 2020.
I did not expect it to run this long; I naively thought we'd come together as a people to tackle this disease, meet it head on, and crush it. We had a common enemy we could rally against, something that could unite us.
Well, here we are two years later. We have made some advancements that are impressive; the mRNA vaccine technology has surpassed our wildest expectations for effectiveness and may lead us to a golden age of health in some respects. For the rest... we still have a long way to go.
---
"More than 3,000 American Covid deaths reported today, 7-day average > 2,500, and the sharp continued rise indicates this peak may exceed that before there were vaccines. Which is unfathomable."
Source:


Commentary: Every death since mid-2021 was preventable. This is a tragedy in the truest sense, because classical tragedy requires a flaw that enables the unfortunate circumstances.
---
What is Omicron? " Just to clarify some confusion about what 'Omicron' is.
'Omicron' has always applied to the whole family (BA.1-3 - we've known about them all since late-Nov/early-Dec).
But the prevalence of BA.1 meant that it got shorthanded as 'Omicron' - that's causing some confusion now!🥴
The first sequences identified were BA.1 - spreading quickly & now coming to dominate.
BA.2 & BA.3 looked a bit like 'little sisters' who weren't as quick - they didn't do much. BA.3 is still not doing much, but BA.2 is now catching up on her sister's heels. 🏃♀️🏃
A call had to be made very early on about whether BA.1 & BA.2 (the most notable) would be given one name or two. There was a lot of discussion of options among scientists. In the end, @WHO decided that all 3 would be called Omicron. "
Source:


Commentary: Omicron refers to the 21M branch of COVID-19, and all indications show that BA.1 and BA.2 are incredibly transmissible. BA.2 probably could have been called Pi instead of Omicron, but regardless, stay masked up.
---
A nasal spray may be on the way that can help reduce spread. "As the SARS-CoV-2 pandemic enters its third year, vaccines that not only prevent disease, but also prevent transmission are needed to help reduce global disease burden. Currently approved parenteral vaccines induce robust systemic immunity, but poor immunity at the respiratory mucosa. Here we describe the development of a novel vaccine strategy, Prime and Spike, based on unadjuvanted intranasal spike boosting that leverages existing immunity generated by primary vaccination to elicit mucosal immune memory within the respiratory tract. We show that Prime and Spike induces robust T resident memory cells, B resident memory cells and IgA at the respiratory mucosa, boosts systemic immunity, and completely protects mice with partial immunity from lethal SARS-CoV-2 infection. Using divergent spike proteins, Prime and Spike enables induction of cross-reactive immunity against sarbecoviruses without invoking original antigenic sin."
Source: https://www.biorxiv.org/content/10.1101/2022.01.24.477597v1
Commentary: This is important research, especially if the nasal spray is temperature stable. While it may not generate primary immunity like the vaccine, it can generate effectively booster-level immunity AND shut down transmission in the nose and throat. Shutting down transmission - especially with variants like Omicron - is essential for long-term success against the SARS-CoV-2 family.
---
A reminder of the simple daily habits we should all be taking.
1. Wear the best mask available to you when you'll be around people you don't live with, even after you've been vaccinated. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Verify your mask's NIOSH certification here: https://www.cdc.gov/niosh/npptl/usernotices/counterfeitResp.html
3. Get vaccinated as soon as you're able to, and fulfill the full vaccine regimen, including boosters. Remember that you are not vaccinated until everyone you live with is vaccinated. If you received an adenovirus vaccine (J&J/AstraZeneca), consider getting an mRNA single shot booster (Pfizer/Moderna) if available. If it's available, choose Moderna as your first choice for both vaccine and booster, Pfizer as your second choice. However, remember than any vaccine is better than no vaccine.
4. Wash/sanitize your hands every time you are in or out of your home.
5. Stay out of indoor spaces that aren't your home and away from people you don't live with as much as practical. Minimize your contact with others and avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
6. Aim to have 3-6 months of living expenses on hand in case the pandemic gives another crazy plot twist to the economy.
7. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
8. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
9. Masks must fit properly to work. Here's how to properly fit a mask:
10. If you think you may have been exposed to COVID-19, purchase a rapid antigen test. This will detect COVID-19 only when you're contagious, so follow the directions clearly. https://amzn.to/3fLAoor
---
Common misinformation debunked!
There is no basis in fact that COVID-19 vaccines can shed or otherwise harm people around you.
Source: https://www.reuters.com/article/factcheck-covid19vaccine-reproductivepro-idUSL1N2MG256
There is no mercury or other heavy metals in the Pfizer mRNA vaccine.
Source: https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no basis in fact that COVID-19 vaccines pose additional risks to pregnant women.
Source: https://www.nejm.org/doi/full/10.1056/NEJMoa2104983
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
Source: https://www.smh.com.au/national/are-we-ignoring-the-hard-truths-about-the-most-likely-cause-of-covid-19-20210601-p57x4r.html
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
Disclosures and Disclaimers
I declare no competing interests on anything I share related to COVID-19. I am employed by and am a co-owner in TrustInsights.ai, an analytics and management consulting firm. I have no clients and no business interests in anything related to COVID-19, nor do I financially benefit in any way from sharing information about COVID-19.
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.