


Lunchtime Pandemic Reading, 24-February-2021
J&J vaccine is safe and effective

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
On schools, from Dr. Gurdasani:
"Brief thread to debunk the repeated claims we hear about transmission not happening 'within school walls', infection in school children being 'a reflection of infection from the community', and 'primary school children less likely to get infected and contribute to transmission'.
I've heard a lot of scientists claim these three - including most recently the chief advisor to the CDC, where the claim that most transmission doesn't happen within the walls of schools. There is strong evidence to rebut this claim. Let's look at this.
Let's look at the trends of infection in different age groups in England first- as reported by the ONS. Being a random survey of infection in the community, this doesn't suffer from the biases of symptom-based testing, particularly important in children who are often asymptomatic
A few things to note:
1. The infection rates among primary & secondary school children closely follow school openings, closures & levels of attendance. E.g. We see a dip in infections following Oct half-term, followed by a rise after school reopening.
We see steep drops in both primary & secondary school groups after end of term (18th December), but these drops plateau out in primary school children, where attendance has been >20% after re-opening in January (by contrast with 2ndary schools where this is ~5%).
Concerningly, the REACT-1 study data released today show that prevalence of infection across England is now highest in primary school children & young adults, with the drops being less steep in primary school children compared to other age groups.
These data are consistent with outbreak data from PHE surveillance, showing that outbreaks in primary schools & pre-school settings continue to occur (albeit at a lower rate than before in primaries), but much more than in secondary schools- in line with higher attendance.
This evidence also feeds into the second myth we hear about - that primary school children don't contribute substantively to transmission. This simply doesn't hold up to scrutiny. The plot from the PHE shows that the number of clusters of cases has been very similar in both.
We also see from the ONS data that primary and secondary school children had the highest prevalence of infection in the community compared to all age groups in December, prior to school closures -prevalence was 2% among primary school children and 3% in 2ndary school children.
All this evidence strongly suggests that infection among children is not simply 'a reflection of infection in the community'. It makes no sense to think that children are getting infected in their households and not within schools.
It's clear that infection in children closely tracks school openings, closure, & the level of attendance. We've seen this in England time and time again. And it's not just secondary schools. It's clear that primary schools play an important role. What about global evidence?
This comprehensive study in Nature Human Behaviour that looked at thousands of interventions implemented at different time points in >200 countries showed that closure of educational institutions was one of the most effective interventions in reducing R.
Ranking the effectiveness of worldwide COVID-19 government interventions
Analysing over 50,000 government interventions in more than 200 countries, Haug et al. find that combinations of softer measures, such as risk communication or those increasing healthcare capacity, ca…
https://www.nature.com/articles/s41562-020-01009-0#MOESM1
But what about the impact of closure of preschool vs primary vs secondary schools. There was no difference- all of them were similarly effective in reducing R- and closure of any setting had a substantial impact on reducing R.
We also have evidence from the UK from our last lockdown in November, when schools were open, and regions where the new variant was dominant (as it is across the UK now) were showing increases in cases (R>1). R in these regions dropped to below 1 only after schools were closed.
This real-world evidence is reflected in recent modelling by LSHTM that also suggests that in almost all scenarios opening primary or secondary schools would lead to rises of R above 1 in England.


It's astonishing that despite all this evidence, the need for mitigatory measures in schools in England has been ignored, and we still promote the myth that primary school settings don't contribute significantly to transmission, and that transmission doesn't happen within schools
We don't have to even look to the 8th of March when the govt is planning to reopen schools. We're having outbreaks in schools now - in preschool & primary school settings. Primary school children have the highest prevalence of infection along with young adults. When will we act?
Want to end on the ONS data on school transmission from last year that showed that primary school children were 2x more likely than adults to be the first case in the household, and once infected, 2x more likely to infect contacts than adults.



This is some of the least biased evidence we have - as it's based on random surveys of children so not dependent on them being symptomatic, and tested. Why are we ignoring this breadth of evidence to the detriment of children, teachers, and communities?"
Source:
Commentary: Despite what folks are saying in order to push for the opening of schools, neither the data nor basic logic supports doing so except in cases where schools have been retrofitted with proper ventilation and the staff has been vaccinated. Simply throwing open the doors without those two precautions is absurdly foolish.
---
What works to shut down COVID-19? A large study in Nature shows the results.
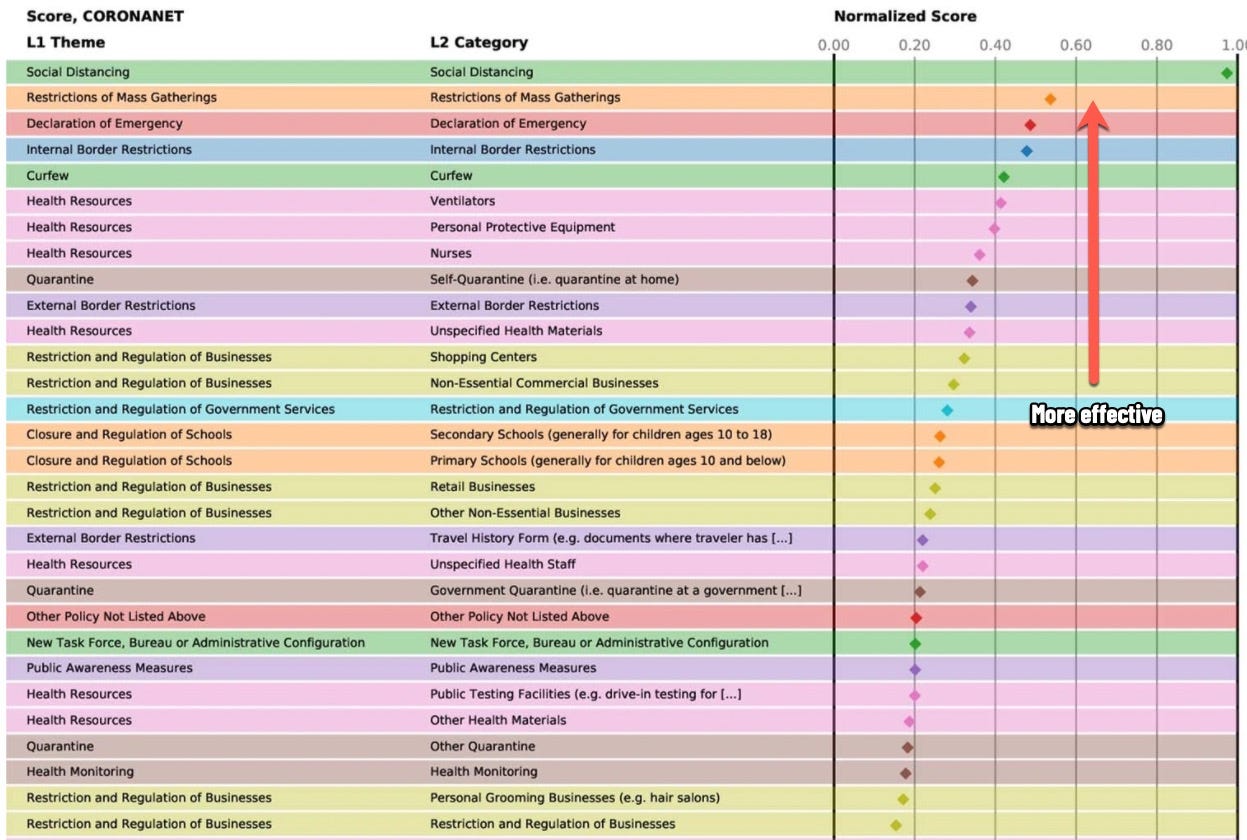
Source: https://www.nature.com/articles/s41562-020-01009-0/figures/6
Commentary: Schools rank above even things like retail businesses and hair salons. They should be classified at the same risk level as non-essential businesses without remediation to prohibit disease spread.
---
J&J vaccine ensemble data is in. "Away we go. J&J ENSEMBLE trial evaluation has landed - 8am again - thanks, FDA! ....1/n
VRBPAC February 26, 2021 Meeting Announcement
This is the CBER Vaccines and Related Biological Products Advisory Committee February 26, 2021 Meeting Announcement.
https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-february-26-2021-meeting-announcement#event-materials
...First up, yes, outcome measure was reasonably close to what we're used to. Here it is based on the FDA-harmonized definition (including mild disease) - & keep in mind this is with South Africa &c included: vaccine efficacy 67% (CI: 56-75) (CI is a measure of uncertainty)...2/n
...This is what that looks like. Keeping in mind it's a single shot - and 28 days after it is about similar to the time of 7 days after BNT-Pfizer's second shot (as they're 3 weeks apart). (ENSEMBLE-2 is underway to see a 2nd shot on day 57) ...3/n
...Severe/critical Covid-19: there's a cut-off date for determining which were severe (adjudication), so could change a bit. Efficacy: 85.4%
(CI 54 to 97) - less certain for aged 60+, with lower numbers: definitely high efficacy, not sure how high though ...4/n
...Hoping to see more later on how severely ill the people were, why they met those criteria. Here's hospitalization: 0 vaccinated people out of over 19,300 after 28 days. Numbers a bit small here. Range of uncertainty for all who tested positive at all: CI 31 to 100 ...5/n
...A post-hoc (unplanned) analysis, looking at hospitalization for who didn't have signs of a previous infection. The 2 vaccinated people hospitalized within 2 weeks were high risk for severe Covid-19...6/n
...7 people died of Covid-19, all in the placebo group, all at high risk of severe outcomes, all in South Africa. 💔
A reminder of the impact of a variant...7/n
... I think this is the first time this very important outcome has been reported for a Covid-19 vaccine trial: all-cause mortality. Wide CIs, so a lot of uncertainty, but 🤞 ... 8/n
...Asymptomatic infection: pic of caveats, not data, because many. They'll have more data over time. Testing for signs of past infection in blood of people who tested negative before vax. Combined that & PCR testing, efficacy against asymptomatic infection 74%
(CI 47 to 88)...9/n
...Vaccine efficacy against moderate/severe Covid-19 was higher in the US: 72% (CI 58 to 82) than Brazil (68%) or SA (64%): over 80% against severe/critical Covid-19 in all 3 countries ...10/n
...Sequencing isn't complete, so they don't have vaccine efficacy rates for variants yet. No one so far had the B.1.1.7 ("UK") or P.1 ("Brazil") variant, but SA is 67% sequenced & 95% were B.1.351 ("SA" variant)...11/n
...Now onto safety & adverse events (AEs). (Reminder I have a backgrounder about what this all means: absolutelymaybe.plos.org/2021/02/21/a-r…)
Like BNT-Pfizer, they have solicited AEs for the first week for a subset. Moderna had them for the whole trial ...12/n
A Reader's Guide to Safety & Adverse Event Data From Vaccine Trials - Absolutely Maybe
The competition for the “honor” of being the most confusing part of clinical trial results is fierce. I don’t think technical terms…
https://absolutelymaybe.plos.org/2021/02/21/a-readers-guide-to-safety-adverse-event-data-from-vaccine-trials/
...Any systemic solicited AE (not injection-related): 55% vax vs 35% placebo; severe <2% vs <1% (that's low). (For Moderna it was 83% vs 53% (bigger injection), 17% severe if previously negative). May be some small under-counting for J&J; FDA said won't make much difference..13/n
...So what were those systemic AEs? Headache, fatigue, myalgia (muscle aches & pains), fever. Severe: Fatigue, myalgia, fever. Rates were higher for younger people (which is so for all of them)...14/n
...Detailed data on duration - I don't think we've had that for any others yet at this level. It was about 2 days. Rates for longer than a week were under 2% & about the same as in the placebo group. On to safety next ...15/n
...Some serious adverse events (SAEs) in people with confounding risk factors, where they could not rule out vaccine involvement: thromboembolic events (clots) & tinnitus (all but one resolving). They considered some cases of hives/swelling as possibly vaccine-related...16/n
...The SAE that resulted in a hold on the trial was a 25-year-old man who had a transverse sinus thrombosis 21 days after vaccine: ultimately determined not to be caused by the vaccine....17/n
...Out of the unsolicited AEs, they considered some (uncommon) likely to be vaccine reactions: arthralgia (joint pain), peripheral neuropathy (numbness or similar in hands/feet); muscle weakness...18/n
...Rate of SAEs similar in vax & placebo groups. FDA judged 3 likely vax-related: 1 allergic reaction (not anaphylaxis); 1 pain from possible injection injury; 1 a severe reaction that resolved in 4 days; plus...19/n
...The FDA couldn't rule out 4 other SAEs, though not likely to be vaccine-related.
There was a reproductive toxicity study (rabbits), which found no problems.
FDA evaluators satisfied on safety & efficacy...20/21
...Single shot, rate of adverse events much lower than mRNAs; high protection from severe Covid-19 & hospitalization; medium-high efficacy against symptomatic disease & possibly asymptomatic; held up against "SA" variant; affordable & low vax costs, non-profit, distributable. /21 "
Source:


Commentary: This is good news on that J&J single shot vaccine. It has fewer side effects, is about 85% effective against severe COVID-19, and holds up against B.1.351. For people outside of high-risk groups, this will probably be the vaccine we receive because of its lower costs and easier distribution.
---
A reminder of the simple daily habits we should all be taking.
1. Always wear the best mask available to you when out of your home and you'll be around other people. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Get vaccinated as soon as you're able to.
3. Wash/sanitize your hands every time you are in or out of your home for any reason.
4. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
5. Get your personal finances in order now. Cut all unnecessary costs.
6. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
7. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
8. Masks must fit properly to work. Here's how to properly fit a mask:
---
Common misinformation debunked!
There is no mercury or other heavy metals in the Pfizer mRNA vaccine. https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.