


Lunchtime Pandemic Reading, 2-October-2020
Inevitable

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
Well, that was only a matter of time. "Trump’s entourage has operated with a casual disregard for coronavirus protocol throughout the pandemic. In August, the president added Scott Atlas, a neuroradiologist with no background in infectious disease, to the Coronavirus Task Force. Atlas proceeded to downplay the virus and meddle with federal testing policy. Upon visiting the White House that month, our colleague Peter Nicholas reported that few West Wing staffers wore masks, and that visitors were not effectively screened for illness. The nation’s most famous address felt “like a coronavirus breeding ground,” he said, because of the lack of safety protocols.
But the president’s illness still raises more questions than it answers. Although Hicks spent considerable time with the president this week, the timing of her illness and of the president’s positive test result may not match up. COVID-19 has a regular course of disease, with a predictable number of days separating infection, early symptoms, and the worst illness. Even the best PCR tests, which detect the virus’s genetic material, are not likely to catch infections that began within the previous two days. In other words, it typically takes four or more days for the virus to multiply and reach detectable levels inside the body.
Someone can test positive for the virus without experiencing symptoms. The Centers for Disease Control and Prevention says that symptoms of COVID-19 are most likely to begin four to five days after exposure, but they have been observed to start anywhere from two to 14 days after exposure. At the same time, current evidence suggests that people who have COVID-19 are most infectious at the very moment their symptoms begin.
Donald Trump is 74 years old, which puts him right on the cusp of the CDC’s riskiest age brackets for COVID-19 outcomes. According to the agency, adults who are 65 to 74 years old are at a higher risk of serious illness, hospitalization, and death than younger people. But adults who are 75 to 84 years old are at much higher risk. The fatality rate for people in Trump’s age cohort, based on the CDC’s most recent age-stratified data, is roughly 8 percent. But for people who are 75 to 84 years old, that rate soars to nearly 18 percent. The president, in other words, is unlikely to die from COVID-19. But the possibility must be acknowledged."
Source: https://www.theatlantic.com/health/archive/2020/10/trump-has-covid-how-bad-could-be/616576/
Commentary: What happens next depends on the virus more than anything. There is still a ton we don't know about its mechanisms in the body in order to predict an outcome for any given single individual.
The simple lesson here: wear a mask, avoid crowds and indoor spaces with others, wash your hands, and watch your distance. The virus ignores your opinion of it or your belief in it.
In terms of timeline, this excellent piece by Katri Manninen gives a good estimate of when to look for outcomes from the prominent folks infected now.
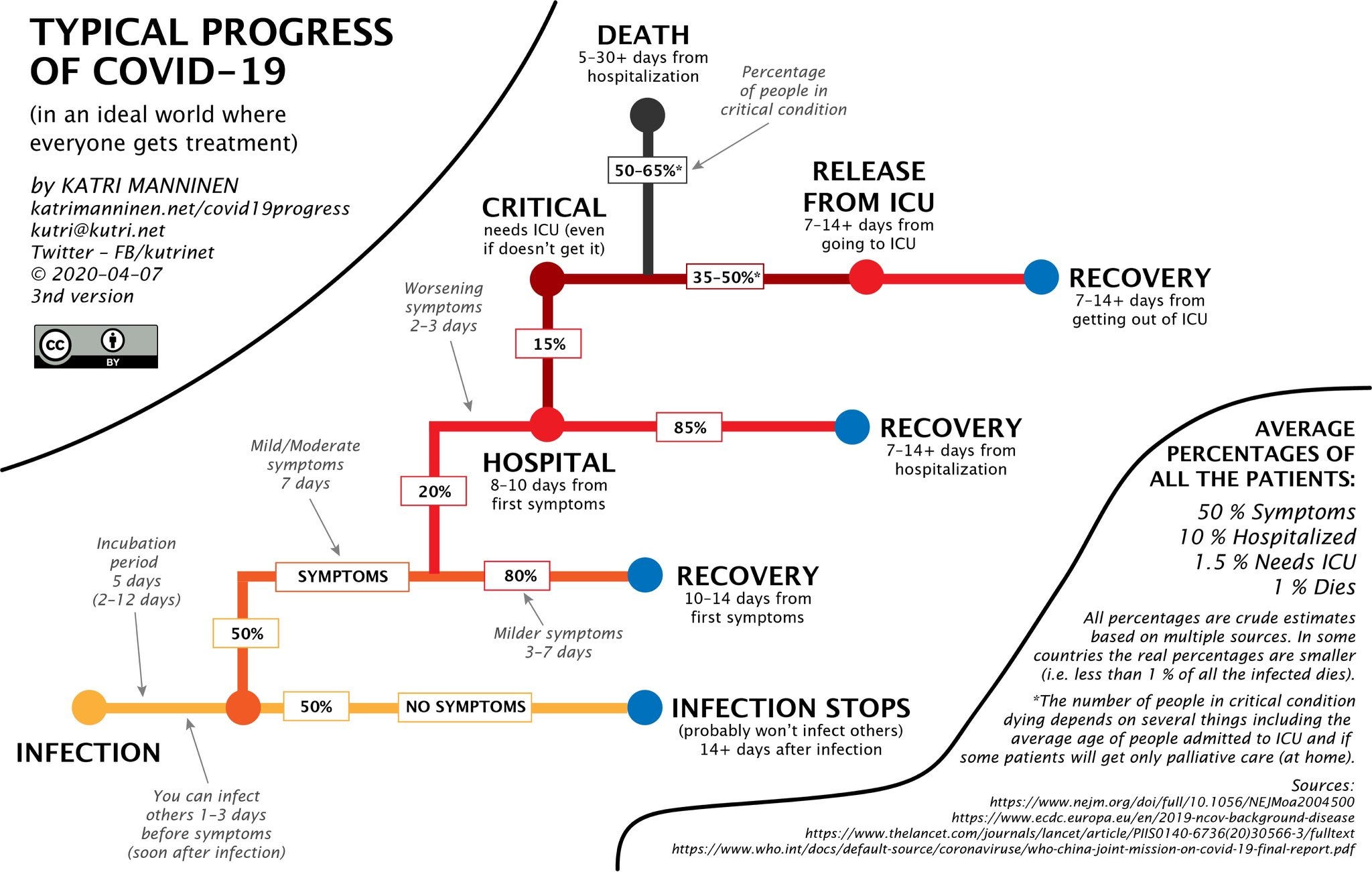
Source: https://katrimanninen.net/covid19progress/
---
An outstanding technical piece on k, the companion metric to R0. "There are COVID-19 incidents in which a single person likely infected 80 percent or more of the people in the room in just a few hours. But, at other times, COVID-19 can be surprisingly much less contagious. Overdispersion and super-spreading of this virus are found in research across the globe. A growing number of studies estimate that a majority of infected people may not infect a single other person. A recent paper found that in Hong Kong, which had extensive testing and contact tracing, about 19 percent of cases were responsible for 80 percent of transmission, while 69 percent of cases did not infect another person. This finding is not rare: Multiple studies from the beginning have suggested that as few as 10 to 20 percent of infected people may be responsible for as much as 80 to 90 percent of transmission, and that many people barely transmit it.
This highly skewed, imbalanced distribution means that an early run of bad luck with a few super-spreading events, or clusters, can produce dramatically different outcomes even for otherwise similar countries. Scientists looked globally at known early-introduction events, in which an infected person comes into a country, and found that in some places, such imported cases led to no deaths or known infections, while in others, they sparked sizable outbreaks. Using genomic analysis, researchers in New Zealand looked at more than half the confirmed cases in the country and found a staggering 277 separate introductions in the early months, but also that only 19 percent of introductions led to more than one additional case. A recent review shows that this may even be true in congregate living spaces, such as nursing homes, and that multiple introductions may be necessary before an outbreak takes off. Meanwhile, in Daegu, South Korea, just one woman, dubbed Patient 31, generated more than 5,000 known cases in a megachurch cluster.
This kind of behavior, alternating between being super infectious and fairly noninfectious, is exactly what k captures, and what focusing solely on R hides. Samuel Scarpino, an assistant professor of epidemiology and complex systems at Northeastern, told me that this has been a huge challenge, especially for health authorities in Western societies, where the pandemic playbook was geared toward the flu—and not without reason, because pandemic flu is a genuine threat. However, influenza does not have the same level of clustering behavior.
We can think of disease patterns as leaning deterministic or stochastic: In the former, an outbreak’s distribution is more linear and predictable; in the latter, randomness plays a much larger role and predictions are hard, if not impossible, to make. In deterministic trajectories, we expect what happened yesterday to give us a good sense of what to expect tomorrow. Stochastic phenomena, however, don’t operate like that—the same inputs don’t always produce the same outputs, and things can tip over quickly from one state to the other. As Scarpino told me, “Diseases like the flu are pretty nearly deterministic and R0 (while flawed) paints about the right picture (nearly impossible to stop until there’s a vaccine).” That’s not necessarily the case with super-spreading diseases."
Source: https://www.theatlantic.com/health/archive/2020/09/k-overlooked-variable-driving-pandemic/616548/
Commentary: Read the whole piece. It emphasizes many different facets of how we think about measuring COVID-19, but it boils down to this: we have to find transmission events, not just individuals infected.
---
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are NEVER to be ingested or injected.
2. Always wear a mask when out of your home and if going to a high risk area, wear goggles. Respirators are back in stock at online retailers, too.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
6. Participate in your local political process. For Americans, go to Vote.org and register/verify your vote.
---
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.