


Lunchtime Pandemic Reading, 19-November-2020
250,000 dead

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
The United States passes the somber milestone of 250,000 dead from COVID-19.
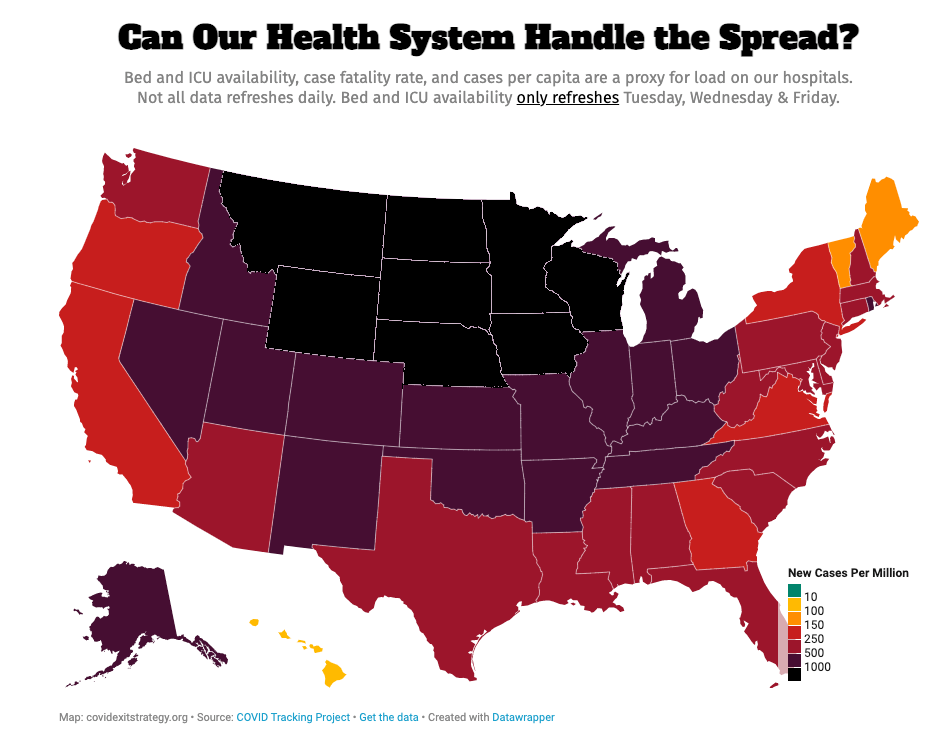
Deaths are spiking because ICUs are out of room and care rationing has begun.
---
Keep your mask up, or you might have trouble keeping something else up. "The COVID-19 pandemic, caused by the SARS-CoV-2, represents an unprecedented challenge for healthcare. COVID-19 features a state of hyperinflammation resulting in a “cytokine storm”, which leads to severe complications, such as the development of micro-thrombosis and disseminated intravascular coagulation (DIC). Despite isolation measures, the number of affected patients is growing daily: as of June 12th, over 7.5 million cases have been confirmed worldwide, with more than 420,000 global deaths. Over 3.5 million patients have recovered from COVID-19; although this number is increasing by the day, great attention should be directed towards the possible long-term outcomes of the disease. Despite being a trivial matter for patients in intensive care units (ICUs), erectile dysfunction (ED) is a likely consequence of COVID-19 for survivors, and considering the high transmissibility of the infection and the higher contagion rates among elderly men, a worrying phenomenon for a large part of affected patients."
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7355084/
Commentary: Sorry not sorry for the crude humor but if there's someone you know who believes in the trope that "wearing a mask is emasculating", COVID-19 will do far worse to them than the mask ever will.

Share among your guy friends to #MaskUp to keep it up. Graphic by the Cleveland Clinic.
---
What does a best-in-class pandemic response look like? Like this:
"After a 2-month period without local transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in China, an outbreak alarm was triggered on October 11, 2020, when three cases of Covid-19 were reported in Qingdao, a coastal city in Shandong Province. Local authorities initiated aggressive contact tracing and quarantine of close contacts of people with confirmed infection. One of the cases initially identified was in a taxi driver who was screened for SARS-CoV-2 as part of routine nucleic acid testing before admission to Qingdao Central Hospital for a transient ischemic attack on October 10. His wife tested positive the next day. She had been working part-time as a nursing assistant at Qingdao Chest Hospital, a facility designated for treating people with imported cases of Covid-19. The third person in this cluster was a man with pulmonary tuberculosis who was treated at the same hospital for 1 month before the outbreak. He was tested at his routine follow-up appointment and was confirmed to be infected with SARS-CoV-2 on October 11. Since the initial epidemiologic evidence suggested that all cases were linked to Qingdao Chest Hospital, the hospital immediately stopped admitting new patients and providing outpatient services.
On the basis of prior experience in Wuhan. opens in new tab and Beijing. opens in new tab, a government task force was established in response to the outbreak. During the week-long holiday after National Day on October 1, many people had visited Qingdao, and the taxi driver’s movements could have led to widespread community transmission. The Qingdao health commission therefore launched a citywide, grid-based mass-screening protocol using reverse-transcriptase–polymerase-chain-reaction (RT-PCR) testing.
Trained medical staff from local hospitals, together with teams dispatched from other cities in Shandong Province, were sent to 4090 testing locations in Qingdao and surrounding suburban areas (see the Supplementary Appendix, available at NEJM.org). Each resident was contacted for testing. Registration information included identity card number, work or residential address, and telephone number. Nasopharyngeal swabs were obtained, and samples were divided into aliquots. To minimize processing time and conserve resources, a pooled testing approach. opens in new tab was used, with each pool containing samples from 3 to 10 people (3 for household contacts of infected people, 5 for hospitalized patients or health care workers, and 10 for community members). If a pooled sample tested positive, individual testing was performed on each person in the pool.
By October 16, a total of 10.9 million people had been tested, and another 9 cases related to the initial cluster were identified using pooled testing, for a total of 12 cases. All testing has now been completed, and no additional cases were found. The outbreak was controlled without a lockdown. Residents were required to wear masks; they were allowed to move freely within the city during the testing process, but they had to have a negative test result before they could use public transportation. People leaving Qingdao also needed to have a negative PCR test result, and most other provincial governments required visitors from Qingdao to quarantine for 1 week and to have a second negative PCR test result before moving freely."
Source: https://www.nejm.org/doi/full/10.1056/NEJMc2032361
Commentary: Three cases led Chinese government officials to test an entire city of 10.9 million people and identify a cluster before it got out of control, leading to only 12 cases in their outbreak.
Obviously, a centrally-controlled, authoritarian government can impose its will on citizens with greater ease than a Western-style democracy. But regardless of government systems, the ability for any government to essentially drop everything and test 10.9 million people in FIVE DAYS is astonishing and shows the speed anyone COULD operate at if they had the resources to do so.
---
One of China's inactivated virus vaccines moves ahead.
"We identified preclinical data on three immunisations using two different doses of CoronaVac (3 μg and 6 μg per dose), an inactivated whole virus vaccine against COVID-19 developed by Sinovac Life Sciences (Beijing, China), providing partial or complete protection in macaques against SARS-CoV-2 challenge, without observable antibody-dependent enhancement of infection. We also identified a phase 2 clinical trial of another inactivated vaccine developed by Sinopharm (Beijing, China), which showed the incidence of adverse reactions was 19·0% within 28 days after two doses of vaccine (5 μg in 0·5 mL of diluent) in a day 0 and 21 vaccination schedule, and the seroconversion rates of the neutralising antibody detected by plaque reduction neutralisation test was 97·6% at 14 days after a day 0 and 21 vaccination schedule. The clinical study of CoronaVac can further provide safety and immunogenic evidence for the inactivated vaccine.
In this first in-human study of CoronaVac, we used a phase 1/2 study design to screen the safety of two doses and two vaccination schedules in a dose-escalation study in a small cohort before expanding the study to a larger cohort to explore the immunogenicity of the vaccine in healthy adults. The immune response in the phase 2 study was substantially higher than in the phase 1 study, which might be due to the difference in preparation process of vaccine batches used in phase 1 and 2 resulting in a higher proportion of intact spike protein on the purified inactivated SARS-CoV-2 virions in the vaccine used in phase 2 than that used in phase 1."
Source: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30843-4/fulltext
Commentary: Each vaccine candidate that we - as a species - create is another arrow in the quiver against SARS-CoV-2 and COVID-19. The more options we have, the better. This is one of the reasons why access to the WHO COVAX project is essential - every nation working together to build a robust, planet-wide response will help us stamp out COVID-19 eventually.
---
One of AstraZenca's vaccines moves ahead. "This study is the fifth published clinical trial of a vaccine against SARS-CoV-2 tested in an older adult population (aged 18–55 years, 56–69 years, and ≥70 years). The vaccine was safe and well tolerated, with reduced reactogenicity in older adults. Antibody responses against the SARS-CoV-2 spike protein were induced in all age groups and were boosted and maintained at 28 days after booster vaccination, including in the 70 years and older group. Cellular immune responses were also induced in all age and dose groups, peaking at day 14 after vaccination.
The populations at greatest risk of serious COVID-19 include people with coexisting health conditions and older adults. The immune correlates of protection against SARS-CoV-2 have not yet been determined, but neutralising antibodies are thought to be associated with protection, and in a COVID-19 non-human primate challenge model, neutralising antibody responses correlated with protection. These findings have led to the use of neutralisation assays to assess immune responses in recent human COVID-19 vaccine trials. Immunisation with ChAdOx1 nCoV-19 results in development of neutralising antibodies against SARS-CoV-2 in almost 100% of participants including older adults without severe comorbidities, with higher levels in boosted compared with non-boosted groups. Further assessment of the efficacy of this vaccine is warranted in all age groups and individuals with comorbidities."
Source: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32466-1/fulltext
Commentary: AstraZeneca's candidate is moving ahead as well, and with good success in older people. Another arrow in the quiver.
---
About that Danish mask study. "Is transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) reduced if most people in a community wear masks? If most people do not wear masks but some do, are the mask wearers protected? These are among the most critical public health questions of this moment, but they are very different questions. In this context, Annals publishes Bundgaard and colleagues' much-anticipated report of DANMASK-19 (Danish Study to Assess Face Masks for the Protection Against COVID-19 Infection), the first randomized controlled trial of a mask recommendation to mitigate SARS-CoV-2 infection (1). We must first emphasize that this trial does not address the first question about transmission in communities where most people wear masks and does not disprove the effectiveness of widespread mask wearing. We explain how this trial adds to what we know about masks in the community and risk for SARS-CoV-2 infection.
Two aspects are important to note. First, the study examined the effect of recommending mask use, not the effect of actually wearing them. Adherence to public health recommendations is always imperfect, as it was in this study, and can differ dramatically in communities with different attitudes toward such recommendations. Second, the effect of a mask recommendation also depends on many other factors, including the prevalence of the virus, social distancing behaviors, and the frequency and characteristics of gatherings. Mask wearing is just one of several interacting strategies to reduce viral transmission, with each reinforcing the others.
The DANMASK-19 findings reinforce the importance of social distancing and hygiene measures and suggest that masks likely need to be worn by most if not all people to reduce community infection rates, which in turn will protect individuals. In the context of observational studies that show lower SARS-CoV-2 transmission in communities with widespread mask wearing (4–7) and the absence of serious adverse health effects of wearing masks (8), the results of this trial should motivate widespread mask wearing to protect our communities and thereby ourselves while we await more definitive evidence during this pandemic."
Source: https://www.acpjournals.org/doi/10.7326/M20-7448
Commentary: The key point here is that masks work best when everyone's wearing them correctly. When only some of the people wear masks, it doesn't work as well because masks are all about source control - stopping the virus coming out of you.
---
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are NEVER to be ingested or injected.
2. Always wear a mask when out of your home and if going to a high risk area, wear goggles. Respirators are back in stock at online retailers, too.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
6. Participate in your local political process. For Americans, go to Vote.org and register/verify your vote.
7. Ventilate your home as frequently as weather and circumstances permit.
---
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.