


Lunchtime Pandemic Reading, 18-July-2022
COVID is much more widespread than you think

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from a qualified healthcare provider who knows your specific medical situation over advice from people on the Internet.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
It's worse than we think by orders of magnitude. "Important to note that case data is hugely undercounting this surge. COVID testing has slowed and shifted to unreported antigen tests. Plots like below can mislead because the current surge looks so much lower than January. But #wastewater data reveals the true levels. (1/4)
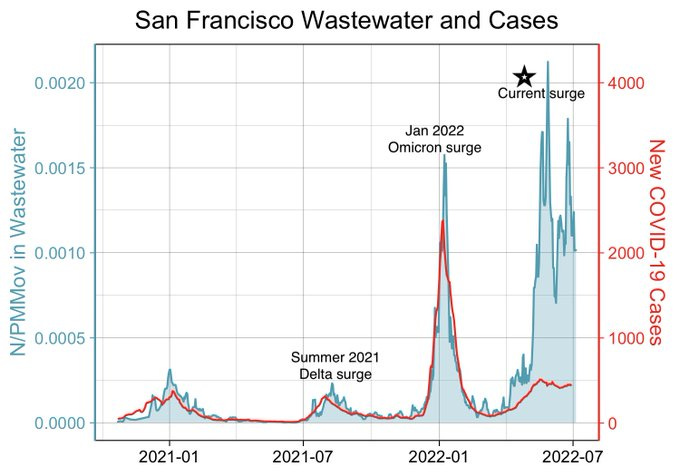
In this example from San Francisco, the concentration of SARS-CoV-2 in wastewater is in blue, and publicly reported cases in red. The red curve might lead you to conclude cases are much lower than in January, but the wastewater values are as high or *higher* than back then! (2/4)"
Source:

Commentary: with positivity rates as high as they are, your best bet to understand the COVID situation in any given location, if it's available, is wastewater data. Why? Because you can't fail to urinate or defecate, COVID-positive or not. It's an aggregate sample that lets you know at the population level what's happening.
---
Long COVID and reinfection. "This graph is a draft for a Long Covid paper I'm working on. The paper will be a while, but I think it's important that people - and policy makers - understand the implications now.
It is *very* serious.
With current estimates of the risk of Long Covid at approx 20% at each infection (yellow line), and policies leading to an expected 2-3 infections per year, **the vast majority of people can expect to have suffered some form of Long Covid within the next 2-3 years**
Even if Long Covid risk is only 10% per infection (grey line), and 2 infections a year, your odds of getting Long Covid reach more than 50% in just over 3 years.
If infection damages your immune system, as several studies suggest, it'll likely happen faster - or be worse.
We don't yet have good data to determine how this risk differs across age, sex, health, genetics and other factors, but given that remains unknown the graph above should scare the living daylights out of Governments, policy-makers, economists ... and you.
Minor correction: 30% is actually 33%, so mislabelled. Hat tip to @ElinBloem for the catch! 🏆
Addendum: This is a *really* simple model. Far more sophisticated modelling can (and hopefully will be) done, however I find more complex modelling is less well communicated. This is a starting point, and not a prediction.
The simple point is this -
Given what we know now, the more times you get infected, the greater the accumulated likelihood you get Long Covid sooner or later. This should be intuitively obvious, but is being ignored by the majority of people and policy makers.
What this actual risk is for different groups, or whether it increases or decreases (or both!) in any subsequent infection is beside this point, as is whether "your" odds are 100% or 10%.
It's rolling the dice, every single time.
And this *will* and *is* having major effects on society.
We cannot continue to ignore it."
Source: This graph is a draft for a Long Covid paper I'm working on. The paper will be a while, but I think it's important that people - and policy makers - understand the implications now.
It is *very* serious.
With current estimates of the risk of Long Covid at approx 20% at each infection (yellow line), and policies leading to an expected 2-3 infections per year, **the vast majority of people can expect to have suffered some form of Long Covid within the next 2-3 years**
Even if Long Covid risk is only 10% per infection (grey line), and 2 infections a year, your odds of getting Long Covid reach more than 50% in just over 3 years.
If infection damages your immune system, as several studies suggest, it'll likely happen faster - or be worse.
We don't yet have good data to determine how this risk differs across age, sex, health, genetics and other factors, but given that remains unknown the graph above should scare the living daylights out of Governments, policy-makers, economists ... and you.
Minor correction: 30% is actually 33%, so mislabelled. Hat tip to @ElinBloem for the catch! 🏆
Addendum: This is a *really* simple model. Far more sophisticated modelling can (and hopefully will be) done, however I find more complex modelling is less well communicated. This is a starting point, and not a prediction.
The simple point is this -
Given what we know now, the more times you get infected, the greater the accumulated likelihood you get Long Covid sooner or later. This should be intuitively obvious, but is being ignored by the majority of people and policy makers.
What this actual risk is for different groups, or whether it increases or decreases (or both!) in any subsequent infection is beside this point, as is whether "your" odds are 100% or 10%.
It's rolling the dice, every single time.
And this *will* and *is* having major effects on society.
We cannot continue to ignore it."
Source:


Commentary: This is key to understanding Long COVID. It's behaving like anything with cumulative exposures, from sunburn to radiation poisoning. The more times you have COVID, the more likely it is you'll contract Long COVID. Whether you've not had COVID or had it multiple times, keep it out of your body!
---
USA COVID positivity rates are at a blistering 42%.
Source: https://www.walgreens.com/businesssolutions/covid-19-index.jsp
Commentary: Positivity rates, as a refresher, are an indication of how good your testing is. If your positivity rates are low - like under 5% - you know you're finding most of the disease in a population. At 42%? The disease is much more widespread than testing can reveal.
---
New escapes. "We studied the prevalent cytotoxic CD8 T-cell response mounted against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Spike glycoprotein269-277 epitope (sequence YLQPRTFLL) via the most frequent Human Leukocyte Antigen (HLA) class I worldwide, HLA A∗02. The Spike P272L mutation that has arisen in at least 112 different SARS-CoV-2 lineages to date, including in lineages classified as ‘variants of concern’, was not recognised by the large CD8 T-cell response seen across cohorts of HLA A∗02+ convalescent patients and individuals vaccinated against SARS-CoV-2, despite these responses comprising of over 175 different individual T-cell receptors. Viral escape at prevalent T-cell epitopes restricted by high frequency HLAs may be particularly problematic when vaccine immunity is focussed on a single protein such as SARS-CoV-2 Spike providing a strong argument for inclusion of multiple viral proteins in next generation vaccines and highlighting the need for monitoring T-cell escape in new SARS-CoV-2 variants."
Source: https://www.cell.com/cell/fulltext/S0092-8674(22)00849-2
Commentary: Right now, our vaccines are calibrated for the spike protein in the SARS-CoV-2 virus. These studies indicate that mutation is occurring elsewhere, making it harder for vaccines to be effective. An analogy is that you have the ability to identify a vehicle by the fact that it has 4 tires, a steering wheel, a seat, an engine, and a body. Now suppose the vehicle has 2 tires. You're no longer able to effectively recognize it. That's what's happening - COVID is mutating further to escape recognition by our immune systems.
---
Vaccination reduces Long COVID risks. "Of 2560 participants, 739 individuals (29%) had COVID-19 (89 asymptomatic), of whom 229 (31.0%; 95% CI, 27.7%-34.5%) had long COVID (Table 1). The prevalence of long COVID varied across the pandemic waves, from 48.1% (95% CI, 39.9%-56.2%) in wave 1 to 35.9% (95% CI, 30.5%-41.6%) in wave 2 to 16.5% (95% CI, 12.4%-21.4%) in wave 3. The number of vaccine doses was associated with lower long COVID prevalence: 41.8% (95% CI, 37.0%-46.7%) in unvaccinated patients, 30.0% (95% CI, 6.7%-65.2%) with 1 dose, 17.4% (95% CI, 7.8%-31.4%) with 2 doses, and 16.0% (95% CI, 11.8%-21.0%) with 3 doses. Older age, higher body mass index, allergies, and obstructive lung disease were associated with long COVID.
With a reference group of unvaccinated females in wave 1 with no allergies or comorbidities (Table 2), male sex (odds ratio [OR], 0.65; 95% CI, 0.44-0.98, P = .04), 2 vaccine doses (OR, 0.25; 95% CI, 0.07-0.87, P = .03), and 3 vaccine doses (OR, 0.16; 95% CI, 0.03-0.84, P = .03) were associated with a lower probability of long COVID. Older age (OR, 1.23; 95% CI, 1.01-1.49, P = .04), allergies (OR, 1.50; 95% CI, 1.06-2.11, P = .02), and an increasing number of comorbidities (OR, 1.32; 95% CI, 1.04-1.68, P = .03) were associated with a higher probability. No statistically significant association with infection wave was found. Among vaccinated individuals (n = 265), time between the second vaccination dose and infection was not associated with long COVID (OR, 0.66; 95% CI, 0.34-1.29)."
Source: https://jamanetwork.com/journals/jama/fullarticle/2794072
Commentary: This is excellent news for folks who are fully vaccinated and a good reminder to keep up with your booster shots.
---
A reminder of the simple daily habits we should all be taking.
1. Wear the best mask available to you when you'll be around people you don't live with, even after you've been vaccinated. P100 respirators are back in stock at online retailers, too and start around US$40 for a reusable respirator. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Verify your mask's NIOSH certification here: https://www.cdc.gov/niosh/npptl/usernotices/counterfeitResp.html
3. Get vaccinated as soon as you're able to, and fulfill the full vaccine regimen, including boosters. Remember that you are not vaccinated until everyone you live with is vaccinated. If you received an adenovirus vaccine (J&J/AstraZeneca), consider getting an mRNA single shot booster (Pfizer/Moderna) if available. If it's available, choose Moderna as your first choice for both vaccine and booster, Pfizer as your second choice. However, remember than any vaccine is better than no vaccine.
4. Wash/sanitize your hands every time you are in or out of your home.
5. Stay out of indoor spaces that aren't your home and away from people you don't live with as much as practical. Minimize your contact with others and avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
6. Aim to have 3-6 months of living expenses on hand in case the pandemic gives another crazy plot twist to the economy, or you know, a global war breaks out.
7. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
8. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
9. Masks must fit properly to work. Here's how to properly fit a mask:
10. If you think you may have been exposed to COVID-19, purchase several rapid antigen tests and/or acquire them from your healthcare provider or government. This will detect COVID-19 only when you're contagious, so follow the directions clearly. https://amzn.to/3fLAoor
---
Common misinformation debunked!
There is no basis in fact that COVID-19 vaccines can shed or otherwise harm people around you.
Source: https://www.reuters.com/article/factcheck-covid19vaccine-reproductivepro-idUSL1N2MG256
There is no mercury or other heavy metals in the Pfizer mRNA vaccine.
Source: https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no basis in fact that COVID-19 vaccines pose additional risks to pregnant women.
Source: https://www.nejm.org/doi/full/10.1056/NEJMoa2104983
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
Source: https://www.smh.com.au/national/are-we-ignoring-the-hard-truths-about-the-most-likely-cause-of-covid-19-20210601-p57x4r.html
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
Disclosures and Disclaimers
I declare no competing interests on anything I share related to COVID-19. I am employed by and am a co-owner in TrustInsights.ai, an analytics and management consulting firm. I have no clients and no business interests in anything related to COVID-19, nor do I financially benefit in any way from sharing information about COVID-19.
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.