


Lunchtime Pandemic Reading, 16-October-2020
8 million

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
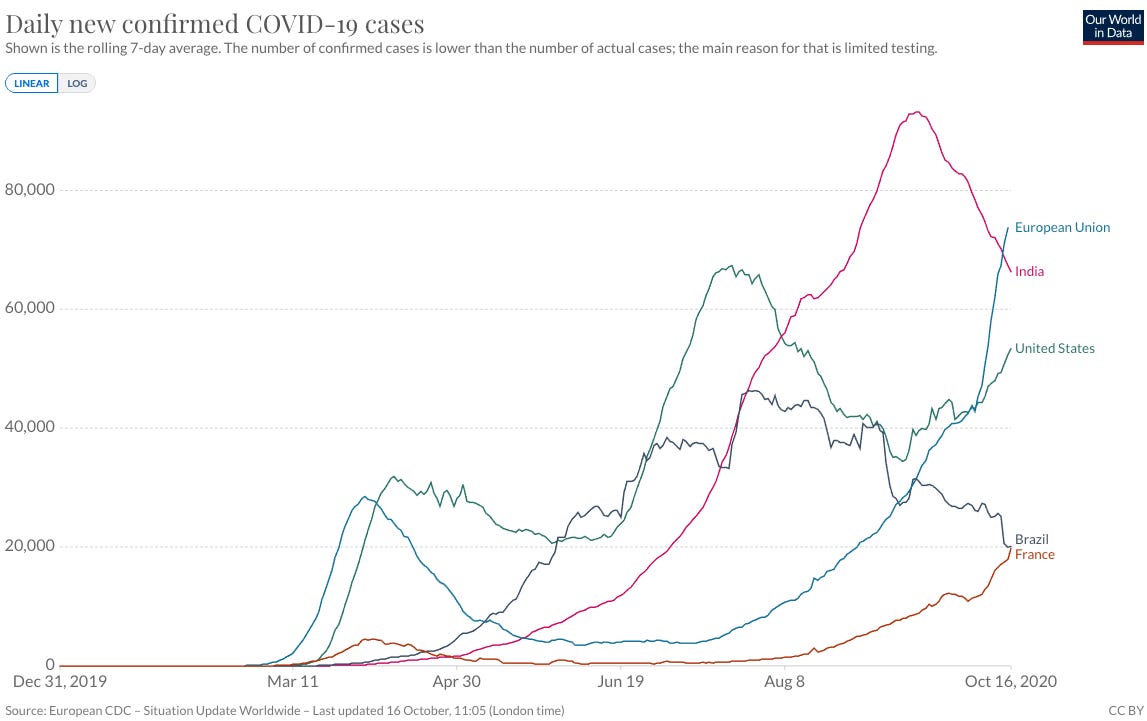
Today, the United States crosses 8 million cumulative cases of COVID-19 and back above 50,000 cases per day, while the EU is headed for 70,000 cases per day and is growing exponentially. The danger that the pandemic presents has not receded or mitigated. It is still a substantial danger to everyone.
---
Inactivated vaccine candidate looks promising. "This is the first report of an inactivated SARS-CoV-2 vaccine tested on human participants. This trial showed that the inactivated SARS-CoV-2 vaccine BBIBP-CorV was safe, tolerable, and immunogenic in healthy people. Two-dose immunisations (on days 0 and 28) at all doses (2 μg, 4 μg, and 8 μg) in two age groups (18–59 years and ≥60 years) induced neutralising antibodies in 100% of vaccine recipients. Mild adverse reactions, including pain and fever, were observed but no severe adverse reaction was reported in all groups.
A vaccine against SARS-CoV-2 is urgently needed to prevent further waves of COVID-19. Immunisation with BBIBP-CorV results in rapid induction of immune responses against SARS-CoV-2, and would be valuable in preventing or limiting the COVID-19 pandemic. Further clinical studies are warranted to evaluate the potential of this vaccine in clinical application."
Source: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30831-8/fulltext
Commentary: Inactivated vaccines are commmonplace; the flu vaccine is one that we've all had experience with. It's good to see them in the clinical trials mix along with the more novel approaches to SARS-CoV-2 even if they're an older technology, because at this point we have no clear idea what will or won't work. The older technology approaches are being used by nations like China that have extensive manufacturing capacity for these kinds of vaccines.
Those nations participating in the WHO CoVax initiative will likely get access to these inactivated vaccines once they pass clinical trials.
---
JAMA asks about allocation of vaccines based on race and prioritizing minorities. "The National Academies of Sciences, Engineering, and Medicine (NASEM) has recommended prioritization of racial minorities who are “worse off” socioeconomically and epidemiologically.1 The World Health Organization (WHO) similarly cautioned that “colorblind” allocation frameworks could perpetuate or exacerbate existing injustices. Both NASEM and WHO urge policy makers to allocate vaccines in ways that reduce unjust health disparities.2 The ethics and legality of race-based policies in the United States have been fraught with controversy.3 This Viewpoint considers how COVID-19 vaccine priority allocations could be implemented ethically and legally.
Compared with the rate of COVID-19–related deaths among non-Hispanic White individuals (mortality rate, 38/100 000) and adjusting for age, the mortality rate relative to population size is 3.4-fold higher among Black individuals (mortality rate, 131/100 000), 3.3-fold higher among Indigenous and Latino communities (mortality rate for both, 125/100 000), 2.9-fold higher among Pacific Islander individuals (mortality rate, 111/100 000), and 1.3 higher among Asian populations (mortality rate, 50/100 000).4 These elevated death rates are unlikely to be explained by biological differences1 but more likely are influenced by social determinants of health, including economic privation and systemic bias. To avoid further compounding these disparities, the NASEM expressly includes “mitigation of health inequities” as 1 of the 3 foundational principles of its framework.1
The NASEM framework allocates vaccines in 4 sequential phases, with distinct priority populations. Within each population group, vaccine access would be prioritized for geographic areas identified as vulnerable through a statistical measure called the Social Vulnerability Index (SVI). The SVI (developed for public health emergencies such as hurricanes or earthquakes) identifies geographic areas of vulnerability based on 15 census variables “most linked to the disproportionate impact of COVID-19 on people of color and other vulnerable populations.”1 The CDC advises state-level planners to draw on the NASEM and the ACIP frameworks, instructing planners to begin identifying “critical populations” including “people from racial and ethnic minority groups.”6 Race, therefore, could be among the explicit factors that health professionals will use to allocate scarce COVID-19 vaccines.
Public health agencies will have considerable discretion in rationing scarce COVID-19 vaccines. They could become agents of change toward improving social and racial justice. Or they can become complicit in allocation strategies that, once again, disproportionately favor the better-off, White majority. Racially neutral approaches must be implemented to advance social and racial justice in the United States."
Source: https://jamanetwork.com/journals/jama/fullarticle/2771874
Commentary: Given how the allocation of EUA and compassionate use emergency drugs has gone - to the wealthy and prominent - it's unfortunately unlikely that vaccine distribution will be any different.
That said, it's worth contacting your legislators, no matter where you live, to urge fair and equitable distribution of therapeutics and vaccines.
---
An amazing, well-researched, and thoroughly disheartening recap of what happens when science takes a back seat to politics. "How the world’s greatest public health organization was brought to its knees by a virus, the president and the capitulation of its own leaders, causing damage that could last much longer than the coronavirus.
ProPublica obtained hundreds of emails and other internal government documents and interviewed more than 30 CDC employees, contractors and Trump administration officials who witnessed or were involved in key moments of the crisis. Although news organizations around the world have chronicled the CDC’s stumbles in real time, ProPublica’s reporting affords the most comprehensive inside look at the escalating tensions, paranoia and pained discussions that unfolded behind the walls of CDC’s Atlanta headquarters. And it sheds new light on the botched COVID-19 tests, the unprecedented political interference in public health policy, and the capitulations of some of the world’s top public health leaders.
Senior CDC staff describe waging battles that are as much about protecting science from the White House as protecting the public from COVID-19. It is a war that they have, more often than not, lost.
Employees spoke openly about their “hill to die on” — the political interference that would prompt them to leave. Yet again and again, they surrendered and did as they were told. It wasn’t just worries over paying mortgages or forfeiting the prestige of the job. Many feared that if they left and spoke out, the White House would stop consulting the CDC at all, and would push through even more dangerous policies.
To some veteran scientists, this acquiescence was the real sign that the CDC had lost its way. One scientist swore repeatedly in an interview and said, “The cowardice and the caving are disgusting to me.”
Collectively, the interviews and documents show an insular, rigorous agency colliding head-on with an administration desperate to preserve the impression that it had the pandemic under control."
Source: https://www.propublica.org/article/inside-the-fall-of-the-cdc
Commentary: This is an outstanding recap of the early days of the pandemic and everything that went wrong and continues to go wrong even today.
---
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are NEVER to be ingested or injected.
2. Always wear a mask when out of your home and if going to a high risk area, wear goggles. Respirators are back in stock at online retailers, too.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
6. Participate in your local political process. For Americans, go to Vote.org and register/verify your vote.
---
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.