


Lunchtime Pandemic Reading, 15-June-2021
US Deep South in deep trouble

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
Patients after kidney transplantation have reduced immune responses. "Patients with kidney failure are at increased risk for SARS-CoV-2 infection making effective vaccinations a critical need. It is not known how well mRNA vaccines induce B and plasma cell responses in dialysis patients (DP) or kidney transplant recipients (KTR) compared to healthy controls (HC). We studied humoral and B cell responses of 35 HC, 44 DP and 40 KTR. Markedly impaired anti-BNT162b2 responses were identified among KTR and DP compared to HC. In DP, the response was delayed (3-4 weeks after boost) and reduced with anti-S1 IgG and IgA positivity in 70.5% and 68.2%, respectively. In contrast, KTR did not develop IgG responses except one patient who had a prior unrecognized infection and developed anti-S1 IgG. The majority of antigen-specific B cells (RBD+) were identified in the plasmablast or post-switch memory B cell compartments in HC, whereas RBD+ B cells were enriched among pre-switch and naïve B cells from DP and KTR. The frequency and absolute number of antigen-specific circulating plasmablasts in the cohort correlated with the Ig response, a characteristic not reported for other vaccinations. In conclusion, these data indicated that immunosuppression resulted in impaired protective immunity after mRNA vaccination, including Ig induction with corresponding generation of plasmablasts and memory B cells. Thus, there is an urgent need to improve vaccination protocols in patients after kidney transplantation or on chronic dialysis."
Source: https://immunology.sciencemag.org/content/6/60/eabj1031
Commentary: This is one of the reasons that even with vaccines, some folks can and should maintain mask protocols, etc. long after vaccination. For immune compromised people, vaccines don't trigger as much of a response, which may mean they will need more booster shots to achieve comparable levels of protection.
---
SARS-CoV-2 hurts us by making us hurt ourselves. "As SARS-CoV-2 has spread around the world, the connections between viral infection, inflammation, and the coagulation cascade have been further illuminated. While the emergent SARS-CoV-2 causes significant disease and death, damage from viral replication appears secondary to exuberant host responses. In an effort to maintain respiratory function, the delicate balance between hemorrhage and fibrosis in the lung is at the nexus of COVID-19 disease. Focusing on the coagulation and fibrinolytic pathways provides a means to evaluate the severity of disease in patients and potentially mitigate its damage with therapeutic treatments. However, preventing the inflammatory cascade that initiates and necessitates the coagulation response may be the only means prevent severe COVID-19 disease. Importantly, these observations of the coagulation pathways may have implications for other infections like influenza or Ebola. Overall, we need a better understanding of the coagulation host response to effectively treat and overcome SARS-CoV-2 and future emergent pathogens."
Source: https://www.jhltonline.org/article/S1053-2498(21)02359-7/fulltext
Commentary: It's interesting that the danger of COVID-19 is the immune system going haywire in the body, rather than the virus being the primary cause of damage. As more research grows, we're gaining a better understanding of how this thing works - critical research because this isn't the first coronavirus we've had to face, and it will not be the last.
---
COVID hangs around in multiple ways. "To our knowledge, this is the first report of long-term (>100 days) persistence of SARS-CoV-2 RNA in lung tissue of an immunocompetent patient after convalescing from COVID-19. The debris-like tissue that contained SARS-CoV-2 RNA might be composed of degenerated endothelial cells that had detached from vessel walls, dysmorphic syncytial elements of pneumocytes, or dead neutrophilic plugs in the interstitium.3, 4 We speculate that this debris-like tissue might shield SARS-CoV-2 RNA from degradation.
Data on sputum, nasopharyngeal swabs, and bronchoalveolar lavage fluid indicate that prolonged detection of SARS-CoV-2 RNA is rare and limited to a few weeks.5 By contrast, SARS-CoV-2 RNA persisted in the lung parenchyma for 105 days after the onset of a mild course of COVID-19. Nonetheless, at the time of writing, 11 months after transplantation, the recipient is in good health. Our data show that the persistence of SARS-CoV-2 RNA in this donor lung tissue has been inconsequential."
Source: https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(21)00240-X/fulltext
Commentary: It's interesting to note how long the virus stuck around in the lung tissue of a healthy individual - 105 days. That's probably indicative of a viral reservoir, which is why the vaccines work so well - they trigger a big alarm instead of being deceived by the virus' relatively quiet alarm it causes in mild cases.
---
How vaccination is going. "But as the map below illustrates, vaccination rates vary widely from state to state, and Southern states, including Louisiana, Alabama and Mississippi showing the lowest rates.
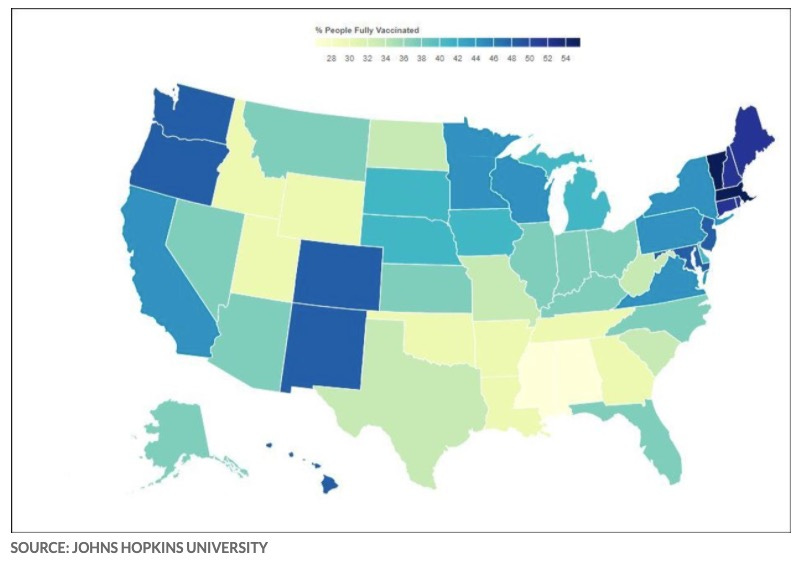
Only Maine, Vermont, Massachusetts, Connecticut and Rhode Island have managed to fully inoculate more than 50% of their populations so far."
Source: https://www.marketwatch.com/story/fears-that-delta-variant-will-become-dominant-covid-strain-worldwide-as-who-says-its-now-in-74-countries-11623768125
Commentary: The Deep South of the USA will be in deep trouble this fall if they don't step up vaccinations, if not sooner. The Delta variant is on a rampage.
Planning to travel? Avoid travel to non-blue states in the map if you have anyone in your party that is not fully vaccinated.
---
A reminder of the simple daily habits we should all be taking.
1. Wear the best mask available to you when you'll be around other people, even after you've been vaccinated. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Get vaccinated as soon as you're able to, and fulfill the full vaccine regimen. Remember that you are not vaccinated until everyone you live with is vaccinated.
3. Wash/sanitize your hands every time you are in or out of your home.
4. Stay home as much as practical. Minimize your contact with others and avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
5. Get your personal finances in order now. Cut all unnecessary costs.
6. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
7. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
8. Masks must fit properly to work. Here's how to properly fit a mask:
---
Common misinformation debunked!
There is no basis in fact that COVID-19 vaccines can shed or otherwise harm people around you.
Source: https://www.reuters.com/article/factcheck-covid19vaccine-reproductivepro-idUSL1N2MG256
There is no mercury or other heavy metals in the Pfizer mRNA vaccine.
Source: https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no basis in fact that COVID-19 vaccines pose additional risks to pregnant women.
Source: https://www.nejm.org/doi/full/10.1056/NEJMoa2104983
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
Source: https://www.smh.com.au/national/are-we-ignoring-the-hard-truths-about-the-most-likely-cause-of-covid-19-20210601-p57x4r.html
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
Disclosures and Disclaimers
I declare no competing interests on anything I share related to COVID-19. I am employed by and am a co-owner in TrustInsights.ai, an analytics and management consulting firm. I have no clients and no business interests in anything related to COVID-19, nor do I financially benefit in any way from sharing information about COVID-19.
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.