


Lunchtime Pandemic Reading, 13-October-2021
J&J + prior COVID

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from a qualified healthcare provider who knows your specific medical situation over advice from people on the Internet.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
J&J + prior COVID has a robust response. "The Johnson and Johnson Ad26.COV2.S single dose vaccine represents an attractive option for COVID-19 vaccination in resource limited countries. We examined the effect of prior infection with different SARS-CoV-2 variants on Ad26.COV2.S immunogenicity. We compared participants who were SARS-CoV-2 naïve with those either infected with the ancestral D614G virus or infected in the second wave when Beta predominated. Prior infection significantly boosts spike binding antibodies, antibody-dependent cellular cytotoxicity and neutralizing antibodies against D614G, Beta and Delta, however neutralization cross-reactivity varied by wave. Robust CD4 and CD8 T cell responses are induced after vaccination, regardless of prior infection. T cell recognition of variants is largely preserved, apart from some reduction in CD8 recognition of Delta. Thus, Ad26.COV2.S vaccination following infection may result in enhanced protection against COVID-19. The impact of the infecting variant on neutralization breadth after vaccination has implications for the design of second-generation vaccines based on variants of concern."
Source: https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(21)00465-0
Commentary: This also hints at the usefulness of a J&J or other booster for those who received the single shot Adenovirus vaccines.
---
What endemic COVID looks like: flu, eventually. "I've meaning to write a "COVID endgame" thread for a while and I apologize this is somewhat delayed compared to media interviews like science.org/content/articl… and statnews.com/2021/09/20/win… and to recent seminars like . 1/17
Here, I've been trying to think about what COVID will look like in its endemic state, ie once the (more or less entire) population has immunity to the virus, blunting transmission and disease relative to the pandemic state. 2/17
I expect endemicity to be achieved at different times throughout the world due to inequities in vaccine distribution and I expect this to be a soft transition rather than a sudden flip of a switch. 3/17
However, even when the entire population of a region has immunity through infection or vaccination, there may still be significant circulation of the virus due to waning immunity and viral evolution. 4/17
As an example, seasonal influenza is an endemic respiratory virus and basically everyone over the age of ~3 will have immunity to it. However, despite this immunity, influenza infects ~10% of the adult population each year and causes perhaps 30k deaths per year in the US. 5/17
Broadly, I expect the eventual endemic state of COVID to be similar with substantial circulation but reduced disease burden relative to the pandemic state. The key parameters here include:
1. R0
2. Waning immunity
3. Antigenic drift
4. Infection to fatality rate (IFR) 6/17
R0 is the average number of secondary infections in a fully naive population. R0 of seasonal flu is around 2. R0 of Wuhan-like SARS-CoV-2 was around 3 and with Delta it's now perhaps 5 or 6. Higher R0 should correspond to greater circulation all other things being equal. 7/17
Waning immunity is a bit more of an open question. Although, other seasonal coronaviruses appear to cause reinfections every ~3 years (nature.com/articles/s4159…), it's hard to completely extrapolate from these viruses to SARS-like coronaviruses. 8/17
But based on what we've observed with waning immunity to infection in SARS-CoV-2, I think it's safe to conclude there will be at least some waning of immunity to infection season-to-season in endemic state. 9/17
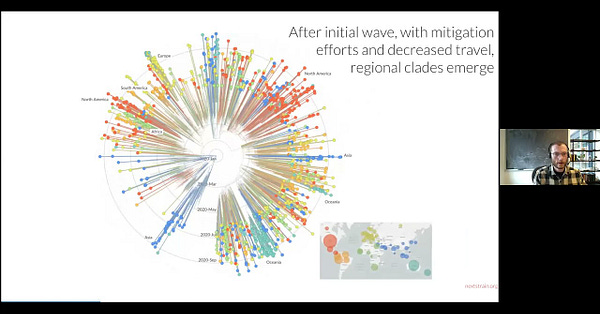
Although so far there's been relatively little antigenic drift in SARS-CoV-2, we've seen rapid adaptive evolution in the S1 domain of spike protein as selection pressure has driven increased transmissibility 10/17
Given the early emergence of partial immune escape in the Beta, Gamma and Mu variants and given the spike protein's observed degree of adaptability, I would suspect that when selection pivots to be primarily immune driven we'll see steady antigenic drift. 11/17
Recent adaptive evolution has been occurring at a significantly faster rate than H3N2 influenza, but my median scenario would be that with switch to endemicity, we see sustained antigenic evolution at a similar pace to influenza H3N2. 12/17
High R0, waning immunity and antigenic drift together suggest substantial seasonal circulation with a speculative guess of 20% or 30% of the population infected each year (often referred to as the "attack rate"). This is higher than flu due to R0 of ~6 rather than ~2. 13/17
At endemicity, circulation does not necessarily translate to disease burden. Based on robust vaccine effectiveness against severe outcomes, my speculative guess would be that infection to fatality rate (IFR) drops 10-fold from its original ~0.6% to a flu-like ~0.06%. 14/17
Together, this would suggest perhaps 40k or 100k deaths per year in the US from COVID at endemic state. Most infections would be relatively mild (just like flu), but there's enough of them that even a small fraction of severe outcomes add up. 15/17
100k deaths would be 30% attack rate with 0.1% IFR, while 40k deaths would be 20% attack rate with 0.06% IFR. In general, like with seasonal flu I would expect significant season-to-season variability. 16/17
This is not cancer or heart disease, but it's still a substantial public health burden. That said, yearly boosters just like flu vaccine, therapeutics like molnupiravir, improved ventilation and rapid testing can all contribute to reducing this ongoing burden. 17/17 "
Source:

Commentary: This is why drug makers are looking at combo shots - COVID, flu, and RSV in one jab. Adopting this would greatly reduce the burden of disease for multiple respiratory diseases in one go. Hopefully we'll see that in a year or two - one-stop shopping for respiratory vaccination.
---
A reminder of the simple daily habits we should all be taking.
1. Wear the best mask available to you when you'll be around people you don't live with, even after you've been vaccinated. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Verify your mask's NIOSH certification here: https://www.cdc.gov/niosh/npptl/usernotices/counterfeitResp.html
3. Get vaccinated as soon as you're able to, and fulfill the full vaccine regimen. Remember that you are not vaccinated until everyone you live with is vaccinated. If you received an adenovirus vaccine (J&J/AstraZeneca), consider getting an mRNA single shot booster (Pfizer/Moderna) if permitted.
4. Wash/sanitize your hands every time you are in or out of your home.
5. Stay out of indoor spaces that aren't your home and away from people you don't live with as much as practical. Minimize your contact with others and avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
6. Aim to have 3-6 months of living expenses on hand in case the pandemic gives another crazy plot twist to the economy.
7. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
8. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
9. Masks must fit properly to work. Here's how to properly fit a mask:
10. If you think you may have been exposed to COVID-19, purchase a rapid antigen test. This will detect COVID-19 only when you're contagious, so follow the directions clearly. https://amzn.to/3fLAoor
---
Common misinformation debunked!
There is no basis in fact that COVID-19 vaccines can shed or otherwise harm people around you.
Source: https://www.reuters.com/article/factcheck-covid19vaccine-reproductivepro-idUSL1N2MG256
There is no mercury or other heavy metals in the Pfizer mRNA vaccine.
Source: https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no basis in fact that COVID-19 vaccines pose additional risks to pregnant women.
Source: https://www.nejm.org/doi/full/10.1056/NEJMoa2104983
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:
There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
Source: https://www.smh.com.au/national/are-we-ignoring-the-hard-truths-about-the-most-likely-cause-of-covid-19-20210601-p57x4r.html
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
Disclosures and Disclaimers
I declare no competing interests on anything I share related to COVID-19. I am employed by and am a co-owner in TrustInsights.ai, an analytics and management consulting firm. I have no clients and no business interests in anything related to COVID-19, nor do I financially benefit in any way from sharing information about COVID-19.
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.