


Lunchtime Pandemic Reading, 12-July-2021
Masks on

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
Mississippi issues new guidance that anyone 65 or older should avoid indoor gatherings regardless of vaccination status. "The rapid rise of Delta variant cases and virus outbreaks combined with the state’s low vaccination rate led the Mississippi Department of Health to release a slew of new COVID-related guidelines on Friday.
The new recommendations, which will stay in place through July 26, are:
All Mississippi residents ages 65 and older, as well as anyone with a chronic underlying medical condition, should avoid all indoor mass gatherings regardless of their vaccination status.
All unvaccinated Mississippians wear a mask when indoors in public settings.
All Mississippians 12 years of age and older get vaccinated. "
Source: https://mississippitoday.org/2021/07/09/msdh-releases-new-guidelines-in-response-to-delta-variant/
Commentary: This is basic math at work. We know from previous studies that vaccines are effective at preventing around 95% of disease for fully vaccinated people with the Pfizer or Moderna vaccines. That drops to 65% against the Delta variant. That's the difference between 1 in 20 people getting a breakthrough infection and 1 in 3 people - a huge difference.
Here's the bottom line: wear the best mask available to you indoors, regardless of vaccination status. Masks kept up safe for the first 16 months of the pandemic. They haven't changed in their effectiveness. Combine them WITH any vaccine and you have a pretty sure bet of safety.
---
The NY Times has some great maps of cases, outbreaks, vaccinations, and most important, risk levels in the USA.
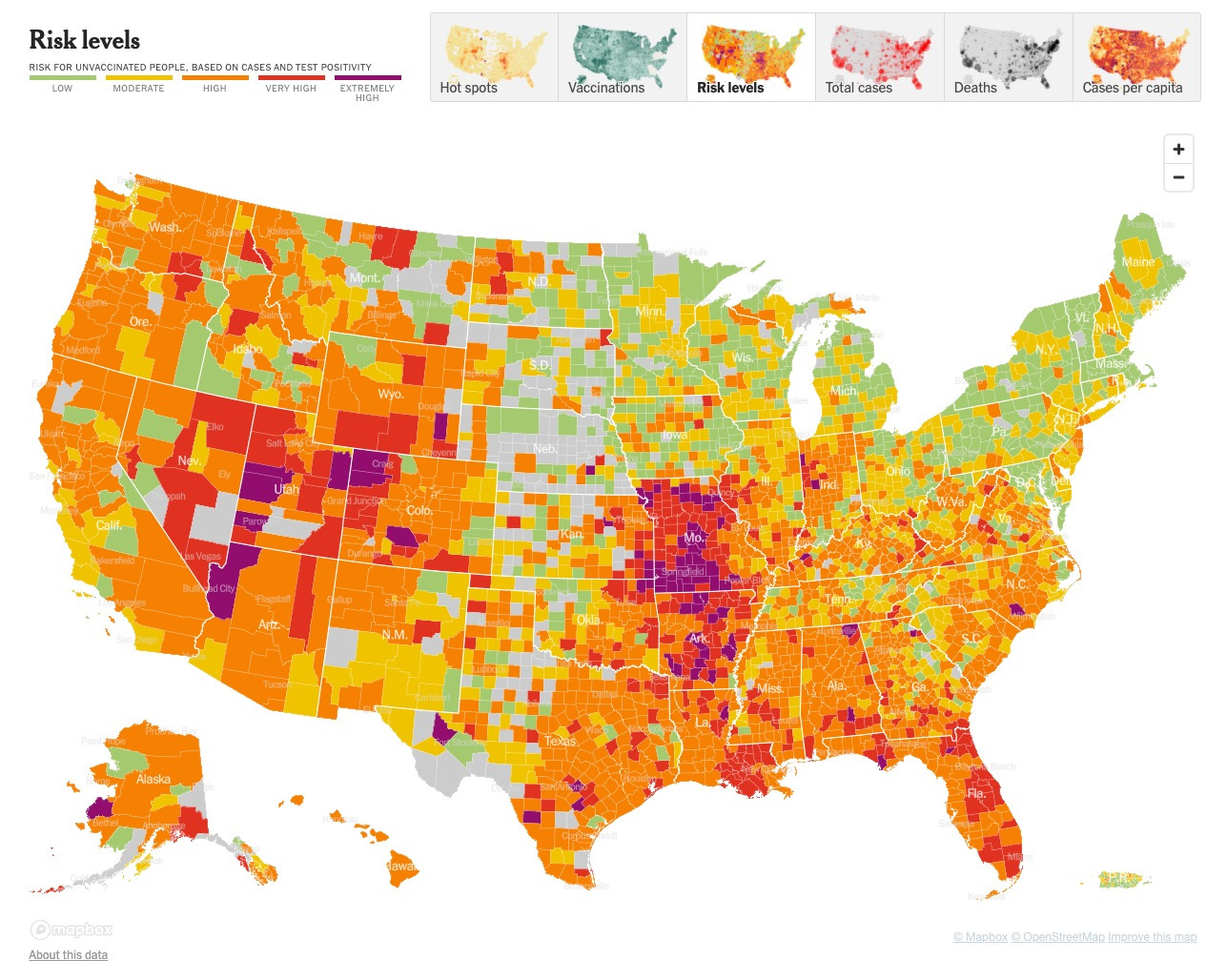
Source: https://www.nytimes.com/interactive/2021/us/covid-cases.html
Commentary: If you're traveling or vacationing in the USA, use this map to judge risk levels. That said, wear a high-quality mask any time you're indoors and you'll be reasonably safe.
---
A new pre-print suggests the risk levels for Delta are indeed more severe. "There were 838 VOC infections in Singapore in the study period. After adjusting for age and gender, B.1.617.2 infection was associated with higher odds of oxygen requirement, ICU admission, or death (adjusted odds ratio (aOR) 4·90, [95% CI 1·43-30·78]. 157 patients with VOCs were admitted to our centre. After adjusting for age, gender, comorbidities, and vaccination, aOR for pneumonia with B.1.617.2 was 1·88 [95% CI 0·95-3·76]) compared with wild-type. B.1.617.2 was associated with significantly lower PCR Ct values and significantly longer duration of Ct value ≤30 (estimated median duration 18 days for B.1.617.2, 13 days for wild-type). Vaccine breakthrough cases were less severe."
Source: https://europepmc.org/article/ppr/ppr356279
Commentary: An 88% increase in severe outcomes for Delta compared to the vanilla SARS-CoV-2 is a big jump in severe outcomes. In effect, it's almost twice as dangerous as COVID-19 was this time last year, though it's good to see vaccines mitigate some of that severity. Mask up. Stay safe. And keep anyone unvaccinated away from other people who aren't vaccinated - and that means kids especially. Don't gamble with their health - Delta is a nasty piece of work.
---
A very long thread from Dr. Trish Greenhalgh on how we got masks so wrong, and why we should have been masking up from the start. Here's the piece:
"When, then, will it be safe for the public to stop wearing masks in indoor spaces? The answer is when there is no longer uncontrolled spread in the community. This US study confirms that if we do it before then, cases are likely to skyrocket. "
Source:

Commentary: The full tweet stream is below.
"LONG THREAD on masks. Mute if not interested.
Do masks work? Why do some people claim they dont work? Do they cause harm? What kinds of masks should we wear? How does masking need to change now we know that Covid is airborne? When can we stop wearing them?
Get your popcorn.
1/
Lets start with observational data. Countries that introduced mandated masking within 30 days of the first case (mostly Asian) had *dramatically* fewer Covid-19 cases than those that delayed beyond 100 days (mostly Western).
https://t.co/J6XOHm1iE0
2/ https://t.co/YitQiYDvSZ
Was this association or causation? Early on in the pandemic, we didnt know. But important point - nobody in these Asian countries seemed to come to harm from wearing a mask.
3/
In this BMJ paper, we presented very limited and indirect empirical evidence (from non-Covid studies) and also *moral evidence* to argue for the precautionary principle: lets all wear masks, *just in case*.
https://t.co/1moaONWaR1
4/
Critics of that early paper were right that the empirical evidence was weak. But they didn't engageand 16 months later have still not engagedwith the moral arguments. They continue to argue that the best course of action in the face of empirical uncertainty is to do nothing.
5/
New drugs & vaccines may have toxic side effects worse than the disease itself. Hence, its appropriate to require definitive empirical evidence from RCTs of the benefit-harm balance before they're introduced. But critics inappropriately applied the same rules to mask studies.
6/
A bit of cloth over the face simply doesnt have the same risks as a novel drug or vaccine, and *doing nothing* could conceivably cause huge harm. Arguing for caution without engaging with the precautionary principle was scientifically nave and and morally reckless.
7/
But thats what happened. Tragically, WHO along with Public Health England, CDC and many other bodies around the world all focused on two things: a) the lack of incontrovertible, definitive evidence and b) speculation about possible harms.
8/
For many mission-critical weeks in early 2020, these bodies persisted in saying theres not enough evidence of benefit and (without evidence) there could be harms, and insisting that these arguments justified inaction.
9/
Asian countries framed the challenge differently. Recalling SARS (2003) and MERS (2012), they werent taking any chances. Masks *might* help in this new disease, so lets wear them just in case. (e.g. Taiwan: https://t.co/1jWEmtMySL)
10/
The most fundamental error made in the West was to frame the debate around the wrong question (do we have definitive evidence that masks work?). We should have been debating what should we do in a rapidly-escalating pandemic, given the empirical uncertainty?.
11/
The putative harms of masks were twofold. First, self-infection. The idea was that the mask was dirty, and by touching it (while putting it on, or when your face itched under it) you might transfer virus to your hands and thence to your eyes etc.
12/
This never made sense. If your mask contains virus, its likely come from you, so youre already infected. There was never any evidence that people touch their faces more when masked. They touch them less.
https://t.co/l2jUQh5990
13/
The meme that *touching your own mask* could kill you was an extraordinary fantasy in which many reputable scientists got swept up. Masking was depicted as a highly specialist activity, dependent on perfect donning/doffing procedures. The public simply werent up to it.
14/
There was an alternative, common-sense view. Your cotton mask is no more likely to kill you than your cotton T-shirt which you pull over your head. In mid-2020, @jeremyphoward came up with the slogan its a bit of cloth, not a land mine.
15/
The other masks-are-harmful meme related to risk compensation. If you wear a mask, youll feel protected and take more risks. Like the driver who becomes more reckless when wearing a seatbelt, youll be slapdash about hand-washing and youll get too close to passers-by.
16/
There was never one jot of evidence for risk compensation. But as Eleni Mantzari and team showed, scientists *talking up* risk compensation as a purely hypothetical problem led to significant negativity towards masks.
https://t.co/TCcDN8So9h
17/
In the name of evidence-based medicine (EBM), the West got off on the wrong foot. We became obsessed with the holy grail of a definitive randomised controlled trial (RCT) that would quantify both the benefits and the harms of masks, just as you would for a drug.
18/
If you were raised in the EBM tradition, where rigorous RCTs are mothers milk, its not easy to get your head round why this was a bad way to approach the problem. Looks like Prof Greenhalgh has lost it, dropped her standards, joined the dark side etc. Bear with me.
19/
A RCT is a controlled experiment. Since people (or animals) are randomly allocated to one or another group (arm), any confounding variables are distributed evenly between the arms so they all cancel out (so long as the study is large enough and allocation is truly random).
20/
Random allocation means that differences between the arms of a RCT are highly likely to be due to the intervention (in this case, masks) and not to confounders. But it does *not* follow that a RCT is better, for any scientific question, than a non-RCT design. Why not?
21/
Many reasons. Drugs are (arguably) a simple intervention, but masks are a highly complex one. As we all know, there are two key questions: do they protect the wearer from other peoples germs and do they protect other people from the wearers germs (source control)?
22/
The RCT design cant cope with this. Its easy to design a study where the primary outcome is infection in wearers, but how would a RCT of source control work? I consent to wearing a mask, but the whole town must consent to be tested (at baseline & repeatedly) for infection.
23/
More fundamentally, were not just interested in whether my mask protects either me or you from catching Covid during a short intervention period (say, one month). Were interested in how masking impacts on the *exponential spread* of an accelerating pandemic.
24/
Take the number 1 and double it, and keep going. 1 becomes 2, then 4, etc. After 10 doubles, you get 512. After 10 more doubles, you get 262144. Now instead of doubling, multiply by 1.9 instead of 2 (a tiny reduction in growth rate). After 20 cycles, the total is only 104127.
25/
=> if masks reduce transmission by a TINY bit (too tiny to be statistically significant in a short RCT), population benefits are still HUGE. UK Covid-19 rates are doubling every 9 days. If they increased by 1.9 every 9 days, after 180 days cases would be down by 60%.
26/
These two issuesthe near-impossibility of using RCTs to test hypotheses about source control and over-reliance on statistically significant effects within a short-term intervention periodis why a RCT of masks is *highly likely to mislead us*.
27/
In short, EBMs preferred methods are unsuited to studying some aspects of the pandemic (notably masks), as is its philosophy of demanding definitive findings and waiting until youve got them.
https://t.co/uwusoI9vjW
28/
Note: as a long-term survivor of a poor-prognosis cancer, I owe my life to RCTs of drugs and surgery. RCTs are fantastic for testing both treatments and vaccines, and have led to many lives being saved in the pandemic. But they are problematic for testing masks.
29/
There havent been many RCTs of masks in the lay public. Its easier to randomise healthcare workers. A few (pre-Covid) RCTs in semi-institutionalised settings (university halls of residence) are summarised here.
https://t.co/UE21yCHuyX
30/
In sum, RCTs of masks were difficult to do, and participants randomised to wearing masks didnt comply well. But these RCTs were in the context of for example a flu outbreak on a university campus in a country that had never seen a deadly pandemic of anything.
31/
The *big Danish mask trial* seemed on very superficial reading - to offer the methodological rigour wed all been waiting for. Its main finding was negative (no significant impact of masks). But it was *fatally flawed* as @dgurdasani1 and I argued):
https://t.co/Ik8G9I8C8I
32/
DANMASK key flaws in one tweet: no CONSORT statement, no ethical approval, inappropriate setting (there was almost no Covid circulating at the time!), under-powered sample, wrong primary outcome, wrong intervention period, inaccurate test, misinterpretation of own findings.
33/
There *never will be* an RCT to tell us definitively whether masks work, because RCTs cant generate dynamic evidence to understand complex interventions in diverse and changing contexts. If youre still looking for effect size = 23% [CI 17-29], youre missing the point.
34/
Yanni Li and colleagues did a meta-analysis of case-control studies. Acknowledging the limitations of such designs, Li et al found that masks reduced SARS-CoV-2 infections by (on average) ~70% in healthcare workers and ~60% in lay people.
https://t.co/FUZy3LJw4y
35/ https://t.co/LcD58AqvbY
Whats a case-control study? Find people who caught Covid and match them with people who were similar but didnt catch Covid; ask whether each was wearing a mask. Relatively weak design because of unmeasured confounders (long story, not going there today).
36/
Hence we need to treat the Li meta-analysis finding with care. On its own, its not definitive; combined with other evidence, it strengthens the case for masks. And another recent case-control study affirms Lis findings.
https://t.co/mtnsULU9x6
37/
Now lets consider observational studies where we measure what happens before and after masking is introduced. These studies may need fancy statistics to correct for confounders (e.g. parallel introduction of lockdown). Some obs studies are pretty flaky; others less so.
38/
Evidence from observational studies (see tweet 2 in this thread) is pretty consistent, though causality is hotly contested. But broadly speaking, in countries and regions where mask mandates were introduced, the rate of spread of the virus subsequently fell substantially.
39/
Lets move on. We need to talk about *mechanistic evidence*. This means evidence from basic science laboratory experiments and real-world case studies for example that helps us understand how the virus spreads and how covering the face *could* work.
40/
Laboratory evidence is often dismissed as low methodological quality by the EBM crowd. Actually, lab studies can be done well or badly (full disclosure: my first doctorate is in lab science). High-quality lab studies are as important as high-quality RCTs.
41/
The idea that a laboratory finding can *contribute* to a scientific conclusion without being stand-alone definitive evidence is important. Masking a complex issue: we amass evidence from different sources: some to help us *understand mechanisms* and some to *test hypotheses*.
42/
Lydia Bourouiba studies how far the stuff that comes out of your mouth and nose when you cough and sneeze travels. Answer: a long way. Common sense says that something placed across the mouth and nose will block some of these flying germs.
https://t.co/UPEig8m3ov
43/
Laboratory simulators can generate clouds of droplets and aerosols (more on those later) similar to a cough. Critics say these arent real conditions. I agree we shouldnt take their quant findings as gospel. But they *add a piece of mechanistic evidence to the jigsaw*.
44/
Heres one lab study for example. Efficiency at reducing the transmission of an artificial respiratory aerosol:
-N95 respirator 99%
-Medical grade mask 59%
-Polyester neck gaiter (single) 47% (double) 60%
-Face shield 2%
https://t.co/55xd0LEHZx
45/
Its time to talk about how this virus spreads. This thread summarises the huge body of evidence that the SARS-CoV-2 virus is airborne. Not just situationally airborne, but floating++ in the air whenever its breathed out.
https://t.co/AvhaEJQIC2
46/
For a long time, WHO and other bodies denied that SARS-CoV-2 was airborne. We wrote a paper on why this error happened (TL;DR: we hypothesised powerful people with entrenched mental models and reputations to lose).
https://t.co/qP4h0g7Fo5
47/
The airborne nature of SARS-CoV-2, now acknowledged by WHO, is a game-changerboth generally and in relation to masks specifically. Generally, we need to avoid close contact (airborne spread occurs *mostly* within 2m), prolonged time indoors, and crowds.
48/
Specifically, we need to shift our mechanistic model from one that focuses on projectile clouds of droplets that come from coughs and sneezes to one that sees the *very air we breathe* as laden with infectious particles. Detail here:
https://t.co/U7FmVDL5sL
49/
There is strong and consistent evidence that (conservatively) 40-50% of all people who catch Covid-19 get it from someone who has no symptoms at the time (i.e. is generating few or no droplets but is just *exhaling* viral-laden air).
https://t.co/YWTQLTJzvQ
50/
March 2020 now seems ancient history. At that time, we were drawing on the Bourouiba study (tweet 43) and similar to argue that *any* bit of cloth over your face would serve as effective source control because it blocked gobby droplets and sneezy droplets.
51/
The large droplet mental model of SARS-CoV-2 transmission also underpinned the argument (so 2020) that masks only work as source control (protecting others but not the wearer). Science has moved on from that position (see below).
52/
If it was all large droplets, masks would work mainly as source control. But given that SARS-CoV-2 travels deep into the lungs in tiny airborne particles, masks need to protect against *inhaling air that others have exhaled*.
https://t.co/z1yoU2XOYs
53/ https://t.co/uGfmWTYNdo
In short, its not coughing and sneezing that spreads this virus so much as breathing and speaking (and also singing) things that generate a lot of aerosols but few droplets.
https://t.co/XAzwKAnF6W
54/
Lets talk about the complex transmission dynamics of SARS-CoV-2, specifically the over-dispersion of R (80% of Covid cases come from only 10-20% of infected people the super-spreaders).
https://t.co/040ClqILEA
55/
Super-spreading individuals (who infect a lot of others) and super-spreading events (where lots of people get infected) are what *drive* the pandemic. Heres a thread of a few.
https://t.co/y6ZiD0bVXT
56/
In a nutshell, we need to *reframe* the key mask research question from what is the effect size of masks on individuals? to how might universal masking impact on the highly non-linear transmission dynamics of this curious virus which behaves VERY differently to flu?.
57/
*This* is why I and others are banging on about masking in public places. If people in England stop wearing masks on so-called Freedom day (19 July), it is highly likely that we will see a vast number of super-spreader events where large numbers of people become infected.
58/
Not only do we need to keep wearing masks, but we need masks that protect us against *airborne transmission* as well as against droplets. Yes its a pain. Yes prolonged masking is a political hot potato bc freedom. But dont shoot the messenger: I didnt invent this virus.
59/
So: What changes do we need to make to our masks to accommodate the fact that Covid is airborne? I want to talk first about lay people and then about the special case of healthcare workers.
60/
There has been a huge amount of research on what makes a perfect mask. In our paper we reviewed 3 factors: how well it filters, how well it fits, and whether you actually wear it (which in turn depends on how comfortable it is).
https://t.co/z1yoU2XOYs
61/ https://t.co/oHO5kUHsMT
Clearly, filtration depends on the material. @cmclase is the expert on this (her early paper here https://t.co/mmrgpJEw9M). She and colleagues have a plain-language website here:
https://t.co/ShcOlQzswj
62/
Clearly, filtration depends on the material. @cmclase is the expert on this (her early paper here https://t.co/mmrgpJEw9M). She and colleagues have a plain-language website here:
https://t.co/ShcOlQzswj
62/
Mask design is now very niche (preprint here), but note: Despite the complexity of the design of a very good mask, it is clear that for the larger aerosol particles, *any* mask will provide substantial protection to the wearer & those around them.
https://t.co/k4R7JgzpcC
63/
Nerdy paper here showing that if you layer different materials in a cloth mask, you can hugely increase the filtration efficiency. But you MUST make sure it fits you and doesnt leak around the edges (see next tweet for tricks).
https://t.co/rI1962umTk
64/
Two tricks to improve the fit of a medical mask: a) wear a cloth mask OVER it (double masking), b) knot the ear loops before going round your ears. (I have a third: use a section of old tights / panty hose instead of the cloth in (a)).
https://t.co/HUzNV3KriL https://t.co/7R5LTM61k0
So if youre not a healthcare worker you can get a lot of protection by pimping a cloth or medical mask, though you may prefer to go for a higher-grade respirator mask. Useful review by @davidshukmanbbc:
https://t.co/H8PR9UjZsu
66/
@davidshukmanbbc What about valves in respirators? Respirators were designed to protect healthy healthcare workers from germs breathed out by patients. The valve was there to make breathing easier. But if the HCW is infected, the valve acts as an exhaust pipe, releasing virus into the air.
67/
@davidshukmanbbc Thats why valved respirators were banned in some public places in 2020. But design has since moved on. *Some* masks and respirators now filter the exhaled air as it passes through the valve, thus removing the virus. Im not plugging any products Google smart respirator.
68/
Now for healthcare workers (HCWs). Big problem here right now. As Ive argued, the SARS-CoV-2 virus is airborne. Airborne virus is a particular problem in hospitals and other healthcare facilities because thats where you go when youre not well.
69/
At the beginning of the pandemic, we talked about aerosol-generating procedures (AGPs) such as intubation, which we thought were the only situations where SARS-CoV-2 became airborne. Heres a thread explaining that tragic error.
https://t.co/bsOGg0X74Q
70/
In short, the only HCWs who were given high-grade protection (including the more efficient respirator masks) were those conducing so-called AGPs. But since *breathing* (especially when unwell) generates aerosols, it makes no sense to have a two-tier protection system.
71/
As I describe in detail in the linked thread from tweet #68, *all* HCWs need to wear respirator masks or some other high-grade protection against aerosols. The refusal of healthcare employers to provide workers with such protection is now a political and legal issue.
72/
Next question: should fully-vaccinated people still wear masks? USA has famously said they dont have to, so lets look at both sides of the argument.
73/
On the one hand, vaccination gives high protection (70-95% depending on the vaccine) against catching the virus and seems to provide similar protection against transmitting it to others.
https://t.co/JvMANRExvP
74/
On the other hand, even 95% protection isnt perfect. It means that if 20 vaccinated people all leave their masks off, thats equivalent to one unvaccinated person. And if were unlucky, one of those 20 people will be a super-spreader.
75/
Whereas masking of HCWs is medical procedure, masking of lay people is a collective cultural activity. It has social significance and moral worth. It conveys messages such as our society is still at risk and I am doing my bit to protect others.
https://t.co/wFwqMtiQ9p
76/
As @zeynep has argued, we wear masks for 3 reasons: to protect ourselves, to protect others, and to model the kind of behaviour that is appropriate in a global pandemic. Creating a vaxd vs unvaxd apartheid will undermine this ethic.
https://t.co/BqUpWgaBHs
77/
What about exercise? Do we really need to wear masks when jogging? The answer is if and only if were getting close enough to share air. So yes, on narrow pavements. Otherwise no.
https://t.co/qha5SFxAJj
78/
Since airborne virus floats away in the outdoors, we usually only need to wear them *indoors*. And the most important settings are where we risk being exposed to high viral loads (i.e. crowded, poorly-ventilated placesespecially hospitals).
https://t.co/pLcasMPZ0O
79/
When, then, will it be safe for the public to stop wearing masks in indoor spaces? The answer is when there is no longer uncontrolled spread in the community. This US study confirms that if we do it before then, cases are likely to skyrocket.
https://t.co/PigZqVdKJU
80/
There are lots of other questions I could have addressed such as masking in kids, more on the politicization of masks, viricidal masks and other novelty designs, future research. But youve probably had enough by now. Ive shared only about 40 papers of 2500.
81/
Thanks to @andreadgibbons @asitmishra @paulglasziou @huffmanlabDU @AndrewsAmbler @originalcoolski @fascinatorfun @PaulWMcCormack @deliman1933 @helenchauhanoz @Paul_Briley @cmclase @seaninsound and others who suggested sources.
82/
END"
---
A reminder of the simple daily habits we should all be taking.
1. Wear the best mask available to you when you'll be around other people, even after you've been vaccinated. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Get vaccinated as soon as you're able to, and fulfill the full vaccine regimen. Remember that you are not vaccinated until everyone you live with is vaccinated. If you received an adenovirus vaccine (J&J/AstraZeneca), consider getting an mRNA single shot booster (Pfizer/Moderna) if permitted.
3. Wash/sanitize your hands every time you are in or out of your home.
4. Stay out of indoor spaces that aren't your home as much as practical. Minimize your contact with others and avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
5. Get your personal finances in order now. Cut all unnecessary costs.
6. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
7. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
8. Masks must fit properly to work. Here's how to properly fit a mask:
---
Common misinformation debunked!
There is no basis in fact that COVID-19 vaccines can shed or otherwise harm people around you.
Source: https://www.reuters.com/article/factcheck-covid19vaccine-reproductivepro-idUSL1N2MG256
There is no mercury or other heavy metals in the Pfizer mRNA vaccine.
Source: https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no basis in fact that COVID-19 vaccines pose additional risks to pregnant women.
Source: https://www.nejm.org/doi/full/10.1056/NEJMoa2104983
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
Source: https://www.smh.com.au/national/are-we-ignoring-the-hard-truths-about-the-most-likely-cause-of-covid-19-20210601-p57x4r.html
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
Disclosures and Disclaimers
I declare no competing interests on anything I share related to COVID-19. I am employed by and am a co-owner in TrustInsights.ai, an analytics and management consulting firm. I have no clients and no business interests in anything related to COVID-19, nor do I financially benefit in any way from sharing information about COVID-19.
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.