


Lunchtime Pandemic Reading, 11-March-2021
Clear masks

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
An easy to read chart of risk levels by age for COVID-19, using data for all of 2020. This illustrates the logic of age-based vaccinations, with and without comorbidities.
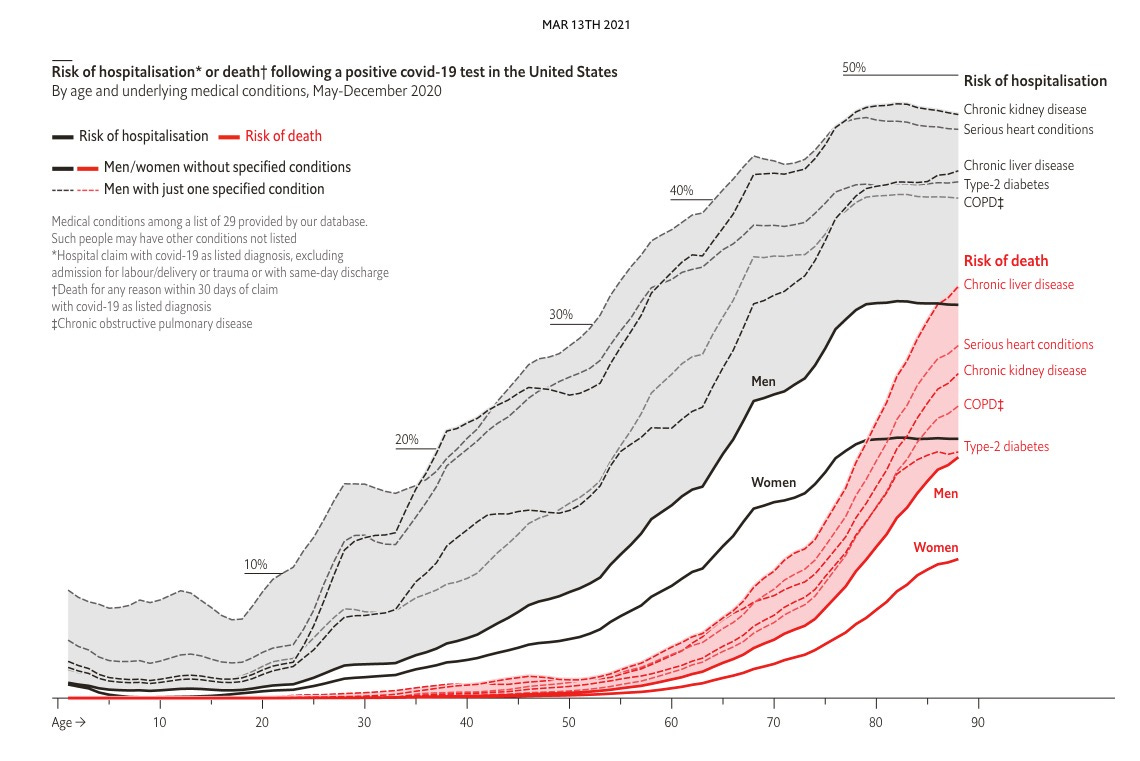
Source: https://www.economist.com/graphic-detail/2021/03/13/our-covid-19-model-estimates-odds-of-hospitalisation-and-death
Commentary: Age is the primary driver, but comorbidities make things many times worse for COVID-19 patients. A vaccine strategy focused on emptying ICUs would follow this chart.
---
Clear masks improve trust. "The primary outcome measures included patient perceptions of (1) surgeon communication and (2) trust in surgeons, as well as (3) quantitative assessments and (4) qualitative assessments regarding patient impressions of the surgeon’s mask. After the clinic encounter, patients completed a verbal survey including validated Clinician and Group Consumer Assessment of Healthcare Providers and Systems questions. Additional questions involved surgeon empathy, trust, and the patient’s impression of the surgeon’s mask. Data were analyzed by comparing patient data in the clear vs covered groups using Cochran-Mantel-Haenszel tests, and comments were analyzed for themes.
Two hundred patients were enrolled from 15 surgeons’ clinics spanning 7 subspecialties. When surgeons wore a clear mask, patients rated their surgeons higher for providing understandable explanations (clear, 95 of 100 [95%] vs covered, 78 of 100 [78%]; P < .001), demonstrating empathy (clear, 99 [99%] vs covered, 85 [85%]; P < .001), and building trust (clear, 94 [94%] vs covered, 72 [72%]; P < .001). Patients preferred clear masks (clear, 100 [100%] vs covered, 72 [72%]; P < .001), citing improved surgeon communication and appreciation for visualization of the face. Conversely, 8 of 15 surgeons (53%) were unlikely to choose the clear mask over their standard covered mask.
This randomized clinical trial demonstrates that patients prefer to see their surgeon’s face. Surgeons who wore clear masks were perceived by patients to be better communicators, have more empathy, and elicit greater trust. Because masks will remain part of the health care landscape for some time, deliberate attention to preserving communication within the surgeon-patient relationship is warranted."
Source: https://jamanetwork.com/journals/jamasurgery/fullarticle/2777511
Commentary: If you work in a profession where empathy is a must, you might want to look at face coverings that offer maximum protection while allowing for full view of the face. These would include systems like powered air-purifying respirators used in welding and construction, designed for hostile environments. They are quite pricey, with four figures in the price tag, but if your profession demands it and you demand maximum protection, these would be the way to go.
---
Mutations continue. "The hazard caused by the emergence of single variants could potentially be contained by polyclonal antibody responses elicited by natural infection, vaccination, or using combinations of monoclonal antibodies in therapeutic interventions. However, the main problem resides in the emergence of new SARS-CoV-2 variants presenting an accumulation of mutations in different Spike domains, creating divergent strains able to evade polyclonal responses. This includes the B.1.1.7 lineage (also known as 501Y.V1 or VOC202012/01), which first emerged in the United Kingdom and has now spread worldwide. Other variants of concern include the B.1.351 lineage (501Y.V2) and the P.1 lineage (501Y.V3), which were first identified in South Africa and Brazil, respectively. These variants have cumulated at least nine non-synonymous mutations/deletions throughout the Spike coding region. Selected mutations were found in the RBM (up to three mutations), including the E484K mutation, identified in vitro in the Liu et al. and Greaney et al. studies. In these concerning variants, RBM modifications are often accompanied with numerous substitutions and/or deletions in the NTD region (up to seven), demonstrating a particular in vivo selective pressure on this site. At least one mutation was also found in the S2 subunit for all three new lineages, confirming the major immune pressure under which the Spike protein evolves. Additional variants are currently under high scrutiny because of the presence of key mutations in the RBM, including the 20A.EU2 variant (S477N), the CAL.20C variant (L452R), and the Danish mink cluster 5 (Y453F). The establishment of sequence monitoring initiatives by public health agencies like the coronavirus disease 2019 (COVID-19) Genomics UK Consortium (COG-UK) are critical to contain the rise of these preoccupying variants by informing and working hand in hand with governments, healthcare systems, and biopharmaceutical companies.
Hopes are now turned toward vaccines that are being deployed globally, which, in conjunction with public health measures, could stop the progression of the COVID-19 pandemic. The immune responses generated by mRNA and adenoviral vector-based vaccines are restricted to the Spike glycoprotein. Thus, their efficacy could be influenced by the emergence of new SARS-CoV-2 Spike variants presenting a major antigenic drift. Recent reports highlighted the deleterious effect of RBM mutations on the neutralization activity of vaccine-elicited antibodies (Wang et al., 2021). One advantage conferred by the mRNA platform is its adaptability and flexibility to rapidly generate new versions accounting for emerging variants. These variants could impact the long-term protective immunity that appears to be elicited by natural infection and vaccination. The emergence of new variants with the distinct capacity to evade polyclonal antibody responses could potentially lead to a growing number of reinfections. In this context, development of second-generation neutralizing antibody cocktails targeting more conserved regions in the RBD or the S2 subunit should be considered, although only a handful of these antibodies have been identified to date. Altogether, these studies shed light on the critical importance of monitoring SARS-CoV-2 sequence variation for a rapid identification of new variants that could require adjustments in vaccine strategies and therapeutic interventions."
Source: https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(21)00089-5
Commentary: The fundamental takeaway here is that everyone, every place, must continue to invest in both testing and genomic sequencing. As vaccines roll out, selective pressure has begun on the virus, which means that mutations will increase as the virus contends with a more hostile environment. Strains will inevitably evolve that offer survival advantage against the first generation of vaccines, so we will be in an arms race with the virus from now on to keep forcing it away.
---
Cancer patients need the full mRNA dosage. "Cancer patients are much less protected against Covid-19 than other people after one dose of the Pfizer vaccine, the first real-world study in this area suggests.
With a 12-week wait for the second dose this could leave them vulnerable, says the King's College London and Francis Crick Institute research team.
An early second dose appeared to boost cancer patients' protection.
Cancer charities are calling for the vaccine strategy to be reviewed.
But Cancer Research UK said the small study had not yet been reviewed by other scientists and people undergoing cancer treatment should continue to follow the advice of their doctors.
The government said it was focused on "saving lives" and the antibody response "was only part of the protection provided by the vaccine".
"The independent Joint Committee on Vaccination and Immunisation (JCVI), which advises government on vaccine use and prioritisation, regularly reviews data and evidence on vaccine efficacy and effectiveness," it said.
About 1.2 million people at very high risk of being seriously ill with Covid-19 were prioritised for a first vaccine dose in the first phase of the UK rollout, which includes people with specific cancers.
The UK government decided to extend the gap between first and second jabs from three to 12 weeks in late December to give more people some protection as soon as possible."
Source: https://www.bbc.com/news/health-56351084
Commentary: While immune-normal people can get away with delaying a second dose of the mRNA vaccines, the same is not true for anyone immune-compromised. If you or someone you know is, work with your healthcare provider to ensure dosages remain on schedule with the vaccine manufacturer's instructions.
---
A reminder of the simple daily habits we should all be taking.
1. Always wear the best mask available to you when out of your home and you'll be around other people. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Get vaccinated as soon as you're able to.
3. Wash/sanitize your hands every time you are in or out of your home for any reason.
4. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
5. Get your personal finances in order now. Cut all unnecessary costs.
6. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
7. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
8. Masks must fit properly to work. Here's how to properly fit a mask:
---
Common misinformation debunked!
There is no mercury or other heavy metals in the Pfizer mRNA vaccine. https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.