


Lunchtime Pandemic Reading, 11-February-2021
Here comes B.1.1.7

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
The fourth surge has begun in the United States as B.1.1.7 spikes. "The increased transmissibility of the B.1.1.7 variant warrants universal and increased compliance with mitigation strategies, including distancing and masking. Higher vaccination coverage might need to be achieved to protect the public. Genomic sequence analysis through the National SARS-CoV-2 Strain Surveillance program will enable a targeted approach to identifying variants of concern in the United States."
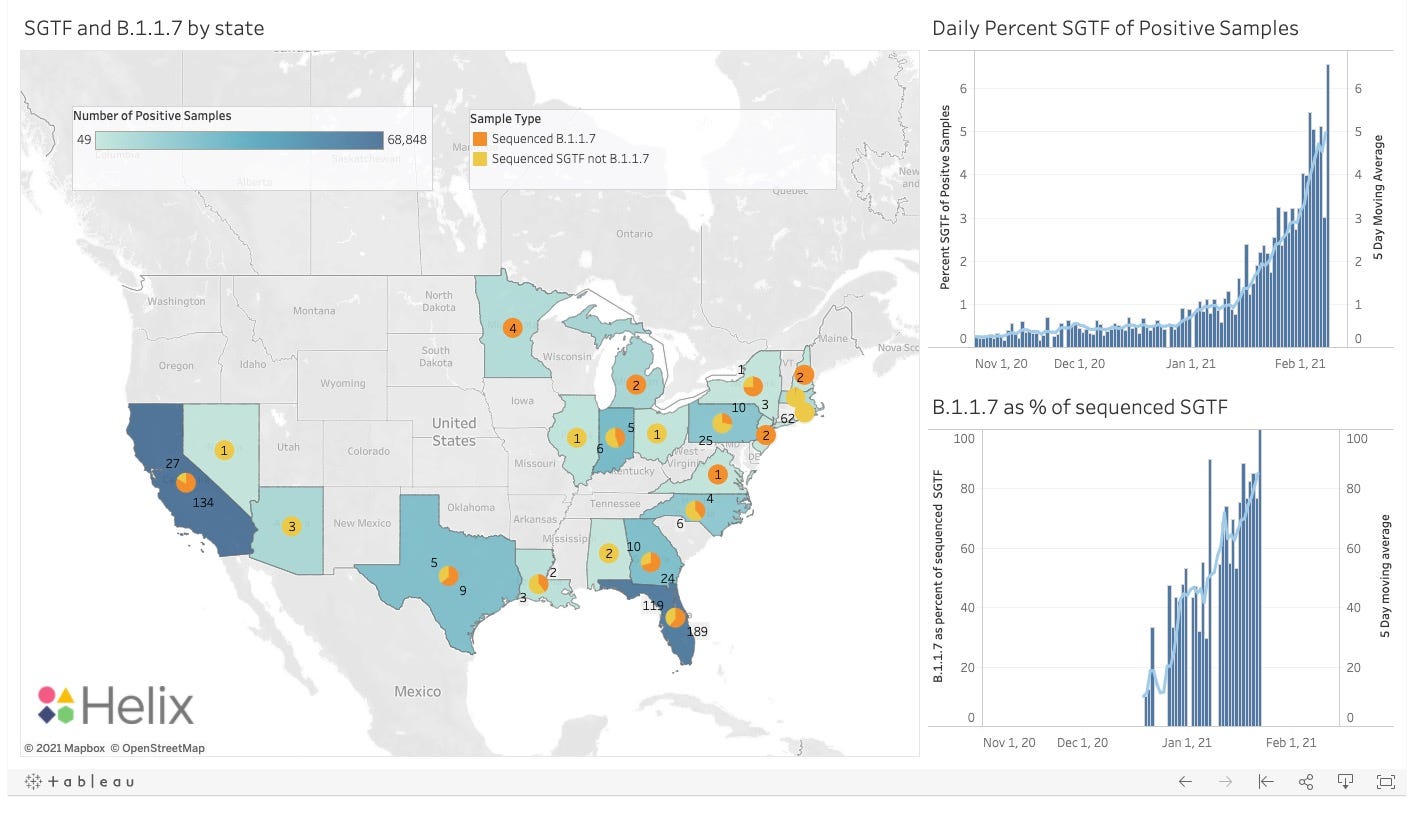
Source: https://public.tableau.com/profile/helix6052#!/vizhome/SGTFDashboard/SGTFDashboard
Source: https://www.cdc.gov/mmwr/volumes/70/wr/mm7003e2.htm
Commentary: What we're seeing here is the new strain, B.1.1.7 gaining dominance in the US population as it did in the UK and Denmark. Our window for shutting it down via distancing measures and vaccination is almost closed; once it becomes the dominant strain, its transmission numbers are much higher than the current SARS-CoV-2 strains, which means our existing measures will not contain it. Cases have dropped off in recent days as new initiatives by the federal government, combined with the absence of major gathering holidays like Christmas, have stunted the virus' spread.
---
Four vaccination challenges. "In the United States, however, public–private health care integration is a state-by-state, county-by-county improvisation, and patients have turned to their health care providers for information about vaccination. To respond to these needs, health care systems are having to master four types of new and unfamiliar work.
The first task is earning the trust of people — both in the public and in the health care workforce — who are reluctant to be vaccinated. Though shrinking, this group is still sizable, particularly in the Black and Latinx communities, which have been disproportionately affected by Covid. The proportion of patients saying they were likely to get vaccinated increased from 39% during the week of October 15, 2020, to 64% during the week of January 3, 2021, according to a survey of 66,818 patients conducted by Press Ganey (where one of us is chief medical officer). Over that period, the proportion saying they were likely to be vaccinated was 60% among White patients but 36% among Black patients.
Vaccine skepticism is not based only on mistrust of systems by communities of color. There is also a core group of people who do not trust any vaccine, joined by skeptics who normally believe in vaccinations but have lost trust in the Food and Drug Administration because of the political pressure it faced to approve vaccines before the presidential election. Strategies and messages may need to be different for each of these groups.
In this context, clinicians have a critical role in addressing vaccine reluctance, in part because of lack of trust in alternative messengers. Between mid-November and early January, only 37% of Press Ganey survey respondents indicated that they had confidence in government advice on vaccination, but 67% said they had confidence in their clinician’s advice.
The second task is managing demand and immunizing people who are ready to be vaccinated. Health care organizations got a taste of the complexity of this task when they began vaccinating employees. In this relatively small population with whom interactions should be reasonably straightforward, organizations had to address the same issues they will face on a much larger scale in vaccinating the public, including communication, prioritization, and management of the vaccinations themselves.
The third task is engaged communication with the public, aiming to go beyond answering “Frequently Asked Questions” to building trust. For example, the community-facing Covid-19 site of Hartford Health has both nationally sourced and locally relevant news items, videos, and podcasts about Covid-related issues, including testing, recovery, and vaccination.5 Patients can sign up for vaccine updates by text. The goal is to provide one-stop shopping for information in various formats and to allow patients to have information pushed to them.
Many of the unknowns can be addressed only by plunging into the fourth task: regional coordination with government and other institutions. Health care providers have had to innovate and improvise to fill the gaps resulting from a long-standing underinvestment in our public health system and the enormity of vaccinating every American rapidly. Working with local government to set up sites for vaccinations at locations such as sports arenas and shopping malls and publicizing prioritization frameworks are two key steps. Another is facilitating information flow. For example, Intermountain Health developed an interoperable interface with the Utah immunization registry that gives clinicians from different health organizations real-time access to its patients’ vaccine information — helping to ensure that people receive their second dose of the right vaccine at the right time."
Source: https://www.nejm.org/doi/full/10.1056/NEJMp2100574
Commentary: Trust, demand, communication, and integration. These challenges apply to every nation, though some have different challenges. China, for example, doesn't need to deal with trust as much because the authoritarian government there can simply mandate citizens receive a vaccine, with substantial penalties for non-compliance.
Here's the key question: what can you do in your community and circle of friends to assist in the mission of getting everyone vaccinated?
---
Comparing measles and COVID-19 when it comes to vaccination. "Today, many Americans express mistrust regarding the safety of Covid-19 vaccines. This attitude is unsurprising in an environment where mask wearing is politicized and loud voices on social media express doubt about the severity — or even existence — of SARS-CoV-2. But the measles vaccine story reminds us that we have an obligation to provide equitable access and clear information; that coordinated, federally supported efforts are essential; and that doubt, distrust, and disinformation can undermine safe, effective vaccines and worthy public health initiatives. Planning for the implementation of SARS-CoV-2 vaccination requires not only working out details of distribution, priority, and cold chains, but also strategies for reaching people who are distrustful, hesitant, dubious, or frankly opposed.5
Protecting children against SARS-CoV-2 infection is both an ethical obligation and a practical necessity. We need data from pediatric trials to reassure parents about the safety and wisdom of this approach. We must prepare for disinformation campaigns that prey on parental fears and target communities made vulnerable through histories of medical neglect, health disparities, and racism. Trusted messengers may help deliver truth and reassurance. And we need to consider lessons from recent measles epidemics — not only about the power of legislative mandates, but also about their potential for sowing distrust if delivered without careful, sensitive, accurate public health messaging. Dare we imagine a campaign that would actually thank children and parents for helping to protect others, as the rubella campaign did, perhaps suggesting that they proudly display their SARS Stars or Corona Diplomas?"
Source: https://www.nejm.org/doi/full/10.1056/NEJMp2034765
Commentary: The key to child vaccination will be pediatric studies, which are underway. Once we know safety and efficacy of the various vaccines in children, we will be able to stop that chain of transmission. Until then - especially with the new strains on the rise - kids will continue to be a risk in any space where they gather. If B.1.1.7 is showing up in your locale, schools should be remote only.
---
COVID-19 tests coming to a phone near you? "A simplified point-of-care assay that turns a smartphone into a fluorescence microscope could expand coronavirus disease 2019 (COVID-19) testing capability, researchers reported in a study in Cell.
The assay, which uses clustered regularly interspaced short palindromic repeats (CRISPR) gene editing technology, emits a fluorescent signal in the presence of the novel coronavirus’s RNA. A smartphone camera can detect this signal directly, without amplification of the viral genome used in most genetic tests. This means the test can quantify the amount of virus in the sample—the quicker the signal is picked up, the higher the viral load.
In the study, the assay was able to detect RNA extracted from patients’ nasal swabs within 5 minutes. Samples with less virus could be detected within 30 minutes. “Monitoring viral loads quantitatively would allow estimation of infection stage and help predict infectivity, recovery, and return from quarantine in real time,” the authors wrote.
“We plan on applying for [Emergency Use Authorization] in the next few months,” researcher Melanie Ott, MD, PhD, of the Gladstone Institute of Virology at the University of California, San Francisco, wrote in a January email. A rollout in pharmacies and drop-in clinics is planned first, with an at-home test potentially to follow later. The technique targets different parts of the virus’ genome, which should make it less vulnerable to false-negatives as the pathogen continues to mutate.
For now, the test still requires laboratory equipment and RNA extraction. “In the future, our next assay will cut out the need for laboratory in a single-step assay,” Ott wrote. The research team also includes Jennifer Doudna, PhD, who shares a Nobel Prize in chemistry for developing CRISPR-based gene editing."
Source: https://jamanetwork.com/journals/jama/fullarticle/2776182
Commentary: This is the way we must go if we want rapid, widespread testing. Hopefully this technology will become available quickly and be fully-administered at home. That would be groundbreaking in terms of our ability to detect disease.
And because RNA is RNA, if enough people have the testing platform available, this could be repurposed down the road for other kinds of viral surveillance like influenza.
---
How to test: Toronto's example. "The door-to-door TCHC testing program is part of the city’s efforts to bring testing to vulnerable populations who need it most, breaking down as many barriers as possible, and connecting residents with services like food hampers, prescription drug drop-off and isolation hotels, if they test positive. It’s a model city officials have been scaling up throughout the fall and winter, and hope to build on when more vaccines are finally available for the wider population.
Last November, the city approved a series of targeted outreach initiatives, for enhanced testing and “wraparound supports,” and has partnered with 12 community organizations doing outreach on the ground, Cressy says. In addition to the door-to-door testing TCHC is doing, this includes mobile and pop-up testing in hard-hit neighbourhoods and connecting people with programs and services like the isolation hotel, even free resources from the library."
Source: https://www.thestar.com/news/gta/2021/02/11/inside-a-toronto-highrise-where-covid-testing-comes-to-the-door-and-why-it-could-be-a-model-for-vaccination.html
Commentary: This is the way. Bring services to at-risk communities where people can't afford to take time off of work or wait in long lines. Get people tested, get people vaccinated, especially in high-density areas where the risk of contagion is much higher. This is how we bring the pandemic down - by shutting off its ability to spread rapidly in dense populations.
---
A reminder of the simple daily habits we should all be taking.
1. Always wear the best mask available to you when out of your home and you'll be around other people. Respirators are back in stock at online retailers, too. Wear an N95/FFP2/KN95 that's NIOSH-approved or better mask if you can obtain it. If you can't get an N95 mask, wear a surgical mask with a cloth mask over it.
2. Get vaccinated as soon as you're able to.
3. Wash/sanitize your hands every time you are in or out of your home for any reason.
4. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
5. Get your personal finances in order now. Cut all unnecessary costs.
6. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
7. Ventilate your home as frequently as weather and circumstances permit, except when you share close airspaces with other residences (like a window less than a meter away from a neighboring window).
8. Masks must fit properly to work. Here's how to properly fit a mask:
---
Common misinformation debunked!
There is no mercury or other heavy metals in the Pfizer mRNA vaccine. https://www.technologyreview.com/2020/12/09/1013538/what-are-the-ingredients-of-pfizers-covid-19-vaccine/
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.