


Lunchtime Pandemic Reading, 10-August-2020
5 million

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
--
Dr. Scott Gottlieb: "Oh, definitely gonna be somewhere between 200,000 and 300,000. And whether we're closer to 200,000, or closer to 300,000 depends on what we do and how this evolves. We've now had two waves of this epidemic, the New York wave and now the wave through the Sunbelt, with which is receding, although Texas is showing signs of an uptick, at least in the last week, and that needs to be followed closely. We're probably going to have another wave and the concern now is that this has become so pervasive across the country, that it could start to infect more rural communities that have been largely been untouched to date, and probably are a little bit more complacent because they have been untouched, but it's still very vulnerable because the infection hasn't been there. It does, if this does become more pervasive across the country, and it's not just in the urban centers, but also in more rural parts of the country, that's going to be far more difficult to control. If it's more widespread, we're seeing indications of that right now, the wave spreading in the Midwest and the West.
We need to have a degree of humility. Children are not immune to this virus. We have seen bad outcomes. The CDC recently documented 570 cases of the multi system inflammatory syndrome in children. There's more cases that are accruing. we've really seen children die. There's 86 kids who died from this, and thousands that have been hospitalized. And so this is a risk in children. We haven't fully characterize that risk. And we're learning new things about this virus all the time. There has been data in the last few weeks that shows that the virus is having an impact on the hearts of adult patients, causing inflammation and some long term sequelae and cardiac symptoms and adults Previously, we didn't really understand that or know that. And so we're learning a lot about this novel virus all the time. We need to have a degree of humility about the risks we need to try to protect children."
Source:
Commentary: Until testing ramps up and gives a school district the ability to test every student and staff member twice a week, I would not personally feel comfortable sending my child to school. That's the heart of the matter: the lack of testing means we don't have proof the virus is or is not spreading through any given community.
Remember the statistics rule: absence of evidence is not evidence of absence.
--
How did New Zealand win? "This case study analyses the leadership approach and practices of the New Zealand government, led by Prime Minister Jacinda Ardern, in the response thus far to the COVID-19 pandemic. It reports on how a shared sense of purpose has been established, that of minimizing harm to lives and livelihoods, for which the government has sought – and secured – New Zealanders’ commitment. Key leadership practices comprise the government’s willingness to themselves be led by expertise, its efforts to mobilise the population, and to enable coping, all of which serve to build the trust in leadership needed for transformative, collective action such as the pandemic demands. At the time of writing, New Zealand appears well on track to achieve its ambitious goal of achieving rapid and complete control over the COVID-19 outbreak – not just ‘flattening the curve’ as other countries are struggling to do – at least in part due to these leadership contributions. A framework of good practices for pandemic leadership is offered drawn from this case study, in the hope transferable lessons can be taken to aid others in the continuing struggle to limit the harm COVID-19 poses to lives and livelihoods throughout the world."
Source: https://journals.sagepub.com/doi/full/10.1177/1742715020929151
Commentary: What makes the cases where countries have beaten COVID-19 easy to understand is this: solidarity. Unified effort. Everyone focused on a single goal, and everyone making the achievement of that goal a priority. That's how you win anything - a world war, a pandemic, landing a person on the moon.
--
Which face masks are better? Pretty much anything is better than nothing, but this study does a fantastic investigation. Fitted N95 is obviously the best, but surgical is a close second, following by many of the cloth ones. Even a single layer cotton cloth mask is pretty good. "Mandates for mask use in public during the recent COVID-19 pandemic, worsened by global shortage of commercial supplies, have led to widespread use of homemade masks and mask alternatives. It is assumed that wearing such masks reduces the likelihood for an infected person to spread the disease, but many of these mask designs have not been tested in practice. We have demonstrated a simple optical measurement method to evaluate the efficacy of masks to reduce the transmission of respiratory droplets during regular speech. In proof-of-principle studies, we compared a variety of commonly available mask types and observed that some mask types approach the performance of standard surgical masks, while some mask alternatives, such as neck fleece or bandanas, offer very little protection. Our measurement setup is inexpensive and can be built and operated by non-experts, allowing for rapid evaluation of mask performance during speech, sneezing, or coughing."
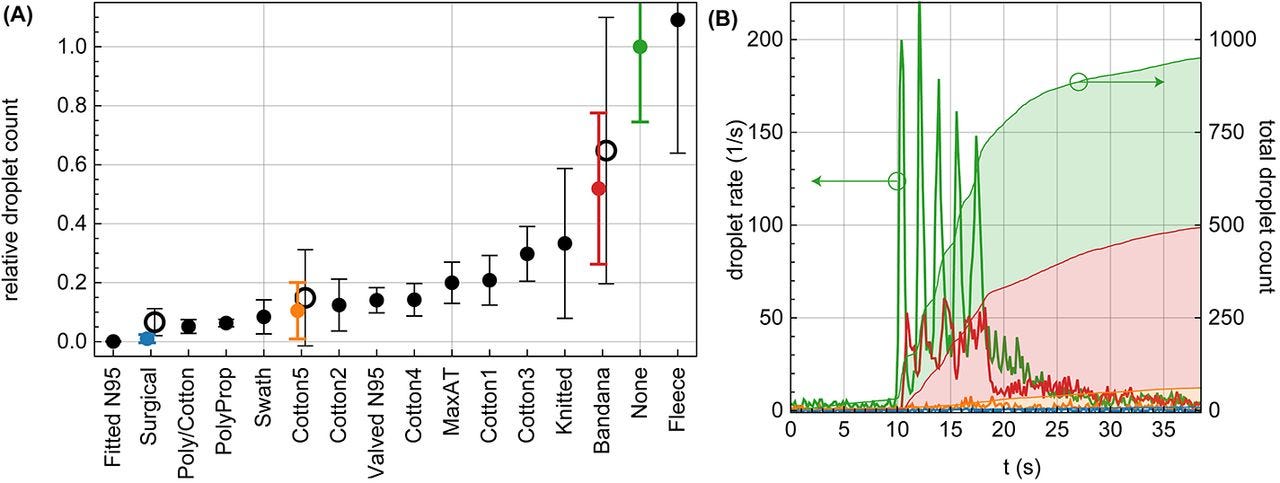
Source: https://advances.sciencemag.org/content/early/2020/08/07/sciadv.abd3083.full
Commentary: Get the best mask you can find and wear it religiously.
--
Brief19 offers caution on a new study that claims flying is safe. "While the math and rationale are compelling, there are several major flaws in this analysis that limit the confidence we can have in the conclusions. The first is that the author assumes that asymptomatic persons are less likely to transmit the disease. This has not been shown to be the case, and in fact many studies suggest that asymptomatic persons can spread the virus as efficiently as those with symptoms. The author believes that asymptomatic people are 40 percent as contagious as symptomatic ones. This is an important assumption that is inadequately supported by available evidence. Secondly, the number of detected infections in each jurisdiction is known be too low. Fortunately, the author corrects by assuming that there are 10 times the number of infections than reported. This is on the high end, but it fairly accounts for a worst-case scenario. But more worrying, the author makes an assumption that contagion only lasts seven days. This is not supported by all available evidence. Many researchers believe that the contagious period for SARS-CoV-2 can in some cases be far longer than that. In addition, the author downplays the potential exposure of lavatory use, and only assumes genuine exposure to people in the same or nearby rows. While air filtration on airplanes is good, making it less likely for a person who coughs in row 15 to infect a person in row 10 or 5 (let alone the opposite direction), the droplet and aerosol features of SARS-CoV-2 remain hotly debated. The very low humidity of airliners may be favorable against spread, but these dynamics simply have not been established for this virus. We’d like to see more possible ranges provided in a final version.
These assumptions and mathematical corrections potentially render the figures reported above as inaccurate. While one of these corrections—the number of infections—might make the numbers seem worse (i.e. make it seem more likely for passengers to encounter an infected person than is really the case), many of these assumptions and corrections dangerously lean in the opposite direction. Therefore, it is possible that the rate of infection from flying is greater than the author of this preprint study has concluded."
Source: https://mailchi.mp/b12cb83a7fc9/your-daily-roundup-from-brief19-5806776?e=87f5efcbeb
Commentary: I would agree with the assessment by the physicians. The model has too many assumptions based on poor or incomplete evidence.
--
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are never to be ingested or injected.
2. Wear a mask when out of your home and if going to a high risk area, wear goggles. Respirators are back in stock at online retailers, too.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
--
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
--
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.