


Lunchtime Pandemic Reading, 1-October-2020
(USA) Register/verify your vote at Vote.org

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
---
For American readers: have you verified your voter registration? Go to Vote.org and ensure it is correct.
---
Does hydroxychloroquine offer prophylactic benefits for healthcare workers? "In this double-blind, placebo-controlled randomized clinical trial that included 132 participants and was terminated early, there was not a significant difference in reverse-transcriptase polymerase chain reaction–confirmed SARS-CoV-2 incidence between hydroxychloroquine and placebo cohorts."
Source: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2771265
Commentary: At this point, the horse we're beating is not only dead, it's chunky salsa, but the fact remains true: HCQ offers no benefit to any part of COVID-19 treatment. Reserve it where it's needed, for the diseases it actually treats.
---
Alcohol usage has increased. "The current analytic sample includes 1540 adults (87.0%; mean [SD] age, 56.6 [13.5] years; 825 [53.6%] were in the age range of 30-59 years; and 883 [57.3%] were female) from the baseline survey who, approximately 1 year later, completed the wave 2 survey (Table 1). Frequency of alcohol consumption increased (1) overall, 0.74 days (95% CI, 0.33-1.15 days), representing an increase of 14% over the baseline of 5.48 days in 2019; (2) for women, 0.78 days (95% CI, 0.41-1.15 days), representing an increase of 17% over the 2019 baseline of 4.58 days; (3) for adults age 30 to 59 years, 0.93 days (95% CI, 0.36-1.51 days), an increase of 19%; and (4) for non-Hispanic White individuals, 0.66 days (95% CI, 0.14 to 1.17 days), an increase of 10% over the 2019 baseline of 6.46 days (Table 2). On average, alcohol was consumed 1 day more per month by 3 of 4 adults. For women, there was also a significant increase of 0.18 days of heavy drinking (95% CI, 0.04-0.32 days), from a 2019 baseline of 0.44 days, which represents an increase of 41% over baseline. This equates to an increase of 1 day for 1 in 5 women. For women there was an average increase in the Short Inventory of Problems scale of 0.09 (95% CI, 0.01-0.17 items), over the 2019 average baseline of 0.23, representing a 39% increase, which is indicative of increased alcohol-related problems independent of consumption level for nearly 1 in 10 women.
These data provide evidence of changes in alcohol use and associated consequences during the COVID-19 pandemic. In addition to a range of negative physical health associations, excessive alcohol use may lead to or worsen existing mental health problems, such as anxiety or depression,6 which may themselves be increasing during COVID-19. The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19."
Source: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2770975
Commentary: 41% increase in heavy alcohol usage by women is substantial; overall increased alcohol usage of 14% is also substantial. It's no surprise, but having the data to confirm anecdotal evidence is useful. Be cautious and judicious with alcohol usage; SARS-CoV-2 does inflict mild viral hepatitis in some cases, so having full function in your internal organs is desirable in case you contract it. A drink every now and then won't substantially cause harm, but heavy drinking absolutely will.
And if you or someone you know is drinking as a coping mechanism, see a qualified mental health practitioner. The pandemic is likely to go on for at least another calendar year; avert unhealthy practices sooner rather than later.
---
Who should get the first COVID-19 vaccines in a situation with limited supply? "The study was determined exempt by the University of Minnesota Institutional Review Board and a waiver of informed consent was granted because data were deidentified and questions posed minimal risk to participants. Data were collected through a module included on the AmeriSpeak Omnibus Survey, fielded by NORC using telephone and internet modes from April 23 to 27, 2020. Respondents were members of AmeriSpeak, a probability-based panel designed to be representative of the US household population. The panel recruitment rate is 34.0%.
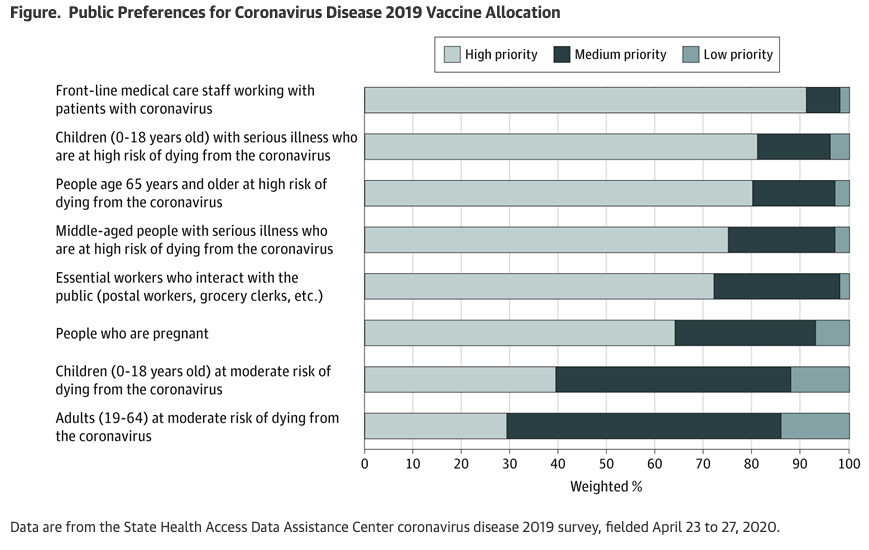
The key measure, adapted from H1N1 public engagement activities in Minnesota,5 described the potential for SARS-CoV-2 vaccine scarcity and that health authorities may have to set guidelines. The survey question asked: “It is anticipated that in the next 12-18 months, a vaccine for coronavirus will be available. However, at least at first, there may not be enough to go around. Public health authorities must set guidelines about who gets the vaccine first. Please indicate the level of priority that should be given for each of the listed groups.” Respondents indicated which of 8 groups (based on age, health risk, and employment type) should receive high, medium, or low priority.
This survey study found that respondents’ preferences were consistent with experts’ emergent recommendations for priority populations for vaccination, suggesting the public would support guidelines that offer vaccine priority to groups defined by age, risk of dying, and employment type.2-4 More than 90% of respondents identified medical workers as high priority. They also rated people at highest risk of dying as higher priority than people with lower risk."
Source: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2770976
Commentary: I'm pleased to see folks have their priorities in order, for who should be protected first, once a working vaccine is available. Even after a vaccine is available - depending on its efficacy - "full normal" is unlikely to return for a while, so plan accordingly.
---
Be wary of any kind of childcare centers. "Young children can contract coronavirus disease 2019 (COVID-19) at childcare facilities and spread the virus to other close contacts, according to findings from a new study from the US Centers for Disease Control and Prevention (CDC). In 3 outbreaks in childcare centers in Utah, the children with infections had mild to no symptoms, and 2 of the children without symptoms likely transmitted severe acute respiratory coronavirus 2 (SARS-CoV-2) to parents, other family members, and possibly their teachers, said the report, which was published in the CDC’s Morbidity and Mortality Weekly Report. Previous studies have found that the infection is less severe in children than adults but that children can nonetheless play a role in transmission.
However, in addition to the outbreaks described in the new CDC report, California’s Sonoma County has reportedly traced an outbreak of at least 30 COVID-19 cases to a student at a childcare center there. According to a September 21, 2020, article in the Los Angeles Times, a county health officer said the center closed for a 2-week quarantine after at least 16 students, 11 relatives, and 3 staff members had tested positive for SARS-CoV-2.
The CDC report describes how researchers used contact tracing data collected between April 1 and July 10, 2020, through Utah’s National Electronic Disease Surveillance System to retrospectively construct transmission chains, identifying 3 outbreaks of COVID-19 at 3 small to large childcare centers in Salt Lake City. They found that in these outbreaks, which were initially linked to 3 index cases of COVID-19 in adults, more than half of the cases eventually linked to the facilities were in children. Of the 22 individuals who likely acquired SARS-CoV-2 infection in the childcare centers, 12 were children, including 9 with mild symptoms and 3 with no symptoms.
The authors of the new CDC study said that mitigation strategies “could have helped limit SARS-CoV-2 transmission in these facilities,” noting that use of masks is recommended for individuals aged 2 years or older. However, they added, some children are too young to wear masks but can transmit COVID-19, as was demonstrated by a child aged 8 months at one of the facilities who transmitted SARS-CoV-2 to both parents. When caring for children too young to wear masks, the authors said, it is especially important that staff members wear a mask themselves, as well as using strategies such as hand washing and frequent disinfection of high-touch surfaces. To help prevent further spread, testing of contacts of people with confirmed COVID-19 cases in childcare centers, including children who might not have symptoms, “could improve control of transmission from child care attendees to family members,” they said."
Source: https://jamanetwork.com/channels/health-forum/fullarticle/2771266
Commentary: If you have a child in a childcare center and you have a realistic option not to, withdraw them. If you have a child in a childcare center without other options, be aware of the heightened risks. Be sure to monitor your child and yourself for symptoms of COVID-19 and obtain testing if possible.
---
Test faster, faster, faster. "It’s time to change how we think about the sensitivity of testing for Covid-19. The Food and Drug Administration (FDA) and the scientific community are currently almost exclusively focused on test sensitivity, a measure of how well an individual assay can detect viral protein or RNA molecules. Critically, this measure neglects the context of how the test is being used. Yet when it comes to the broad screening the United States so desperately needs, context is fundamental. The key question is not how well molecules can be detected in a single sample but how effectively infections can be detected in a population by the repeated use of a given test as part of an overall testing strategy — the sensitivity of the testing regimen.
Thinking about impact in terms of repeated uses is a familiar concept to clinicians and regulatory agencies; it’s invoked every time we measure the efficacy of a treatment regimen rather than a single dose. With Covid-19 cases accelerating or plateauing throughout much of the world, we urgently need to shift our attention from a narrow focus on the analytic sensitivity of a test (the lower limit of its ability to correctly detect small concentrations of molecules in a sample) to the more relevant measure of a testing regimen’s sensitivity to detect infections (the probability that infected persons learn they’re infected in time to be filtered out of the population and prevent spread to others). A point-of-care test that was inexpensive enough to use frequently would have a high sensitivity for detecting infections in time to act, without having to meet the benchmark analytic limit of detection (see diagram).
The Centers for Disease Control and Prevention (CDC) estimated in June 2020 that there were 10 times as many Covid-19 cases in the United States as had been detected.5 In other words, despite very high analytic sensitivity of the diagnostic tests deployed for surveillance, today’s testing regimens have at best only 10% sensitivity to detect infections and are failing as Covid filters.
For an effective Covid filter that will stop this pandemic, we need tests that can enable regimens that will capture most infections while they are still infectious. These tests exist today in the form of rapid lateral-flow antigen tests, and rapid lateral-flow tests based on CRISPR gene-editing technology are on the horizon. Such tests are cheap (<$5), can be produced in the tens of millions or more per week, and could be performed at home, opening the door to effective Covid filter regimens. Lateral-flow antigen tests do not have an amplification step, so their analytic limits of detection are 100 or 1000 times higher than that of the benchmark test, but that is largely inconsequential if the goal is to identify people who are currently transmitting virus. SARS-CoV-2 is a virus that grows quickly inside the body, so by the time a benchmark PCR test becomes positive, the virus is well into exponential growth. At that point, it is probably hours, not days, before the virus grows by orders of magnitude, reaching the detection thresholds of currently available cheap and rapid point-of-care tests. It is after this point, when people would have positive results on both tests, that they would be expected to become infectious (see diagram)."
Source: https://www.nejm.org/doi/full/10.1056/NEJMp2025631
Commentary: Faster results, even with less sensitivity, are essential to stopping the pandemic. Which would you rather have - a smoke detector that's a little too sensitive, or a smoke detector that waits until it's absolutely sure there's a fire? That's where we are with testing right now. We are testing so little, so infrequently, that we're effectively waiting until we're sure there's a fire - and then everything around us is on fire. Better to test much more frequently and have some false positives.
---
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are NEVER to be ingested or injected.
2. Always wear a mask when out of your home and if going to a high risk area, wear goggles. Respirators are back in stock at online retailers, too.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters, preferably more. Avoid indoor places as much as you can; indoor spaces spread the disease through aerosols and distance is less effective at mitigating your risks.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Replenish your supplies as you use them. Avoid reducing your stores to pre-pandemic levels in case an outbreak causes unexpected supply chain disruptions.
6. Participate in your local political process. For Americans, go to Vote.org and register/verify your vote.
---
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:

There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
---
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender-balanced, because multiple, diverse perspectives on research data are essential.