

Lunchtime Pandemic Reading, 2-June-2020
Lunchtime Pandemic Reading, 2-June-2020
Masks, masks, masks

Lunchtime pandemic reading.
Standard disclaimer: this is a roundup of informative pieces I've read that interest me on the severity of the crisis and how to manage it. I am not a qualified medical expert in ANY sense; at best I am reasonably well-read laity. ALWAYS prioritize advice from qualified healthcare experts over some person on Facebook.
This is also available as an email newsletter at https://lunchtimepandemic.substack.com if you prefer the update in your inbox.
You are welcome to share this.
--
Let's get a sense of where we are. This is using Our World in Data's charting software, which is very helpful, especially if you want to scale the data based on population. What we see is that for nations who have implemented strong controls, things are settling down, like a fire inside its containment barrier. For nations with poor controls, disease growth continues. More on containment in a bit.
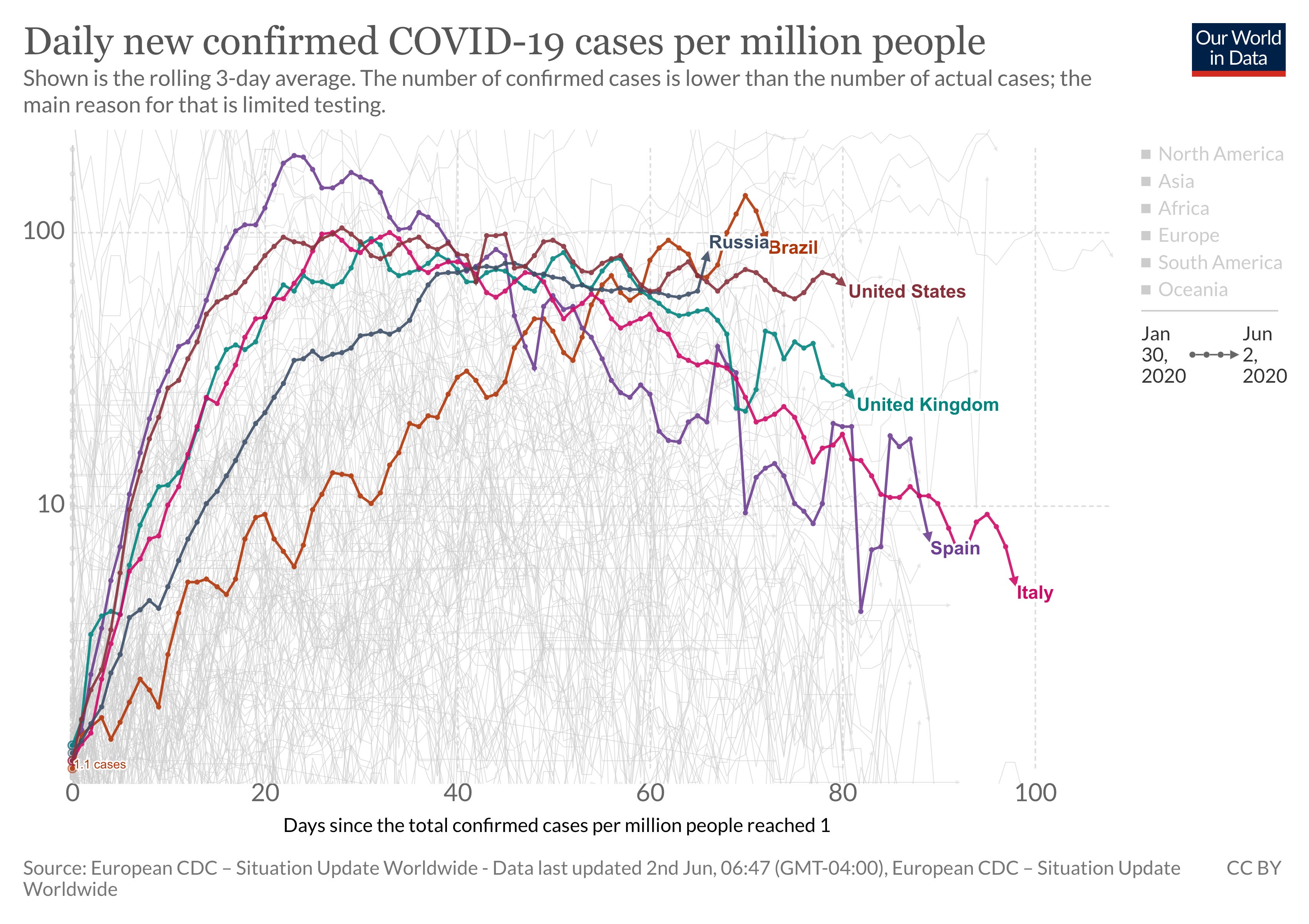
Source: https://ourworldindata.org/coronavirus-data-explorer?yScale=log&zoomToSelection=true&country=USA~BRA~RUS~GBR~ESP~ITA&casesMetric=true&dailyFreq=true&aligned=true&perCapita=true&smoothing=3
--
Viral genetics expert Trevor Bedford on the US cutting ties with WHO: "The US CDC plays a central role in the GISRS network. How is this work supposed to continue? I'm also concerned that SARS-CoV-2 will evolve antigenically over the coming years and we'll need a process to update its vaccine. How are we supposed to do this without the WHO? 8/8"
Source:

Leaving any organization means leaving its resources. Regardless of the politics around WHO, its resources - particularly access to data - are essential for preparing countermeasures for influenza and SARS-CoV-2. I hope future US administrations restore ties to it so that we can continue to benefit from the data available.
--
There may not be a fall rebound of COVID-19... because it might be July. "We can't assume that we are in for a second wave in the fall. We may be in for a second wave in July."
Source:


It's somewhat pointless to talk about a second wave if we've never really emerged from the first one.
--
A meta-analysis in the Lancet confirms current measures. "In view of inconsistent guidelines by various organisations based on limited information, our findings provide some clarification and have implications for multiple stakeholders. The risk for infection is highly dependent on distance to the individual infected and the type of face mask and eye protection worn. From a policy and public health perspective, current policies of at least 1 m physical distancing seem to be strongly associated with a large protective effect, and distances of 2 m could be more effective. These data could also facilitate harmonisation of the definition of exposed (eg, within 2 m), which has implications for contact tracing. The quantitative estimates provided here should inform disease-modelling studies, which are important for planning pandemic response efforts. Policy makers around the world should strive to promptly and adequately address equity implications for groups with currently limited access to face masks and eye protection. For health-care workers and administrators, our findings suggest that N95 respirators might be more strongly associated with protection from viral transmission than surgical masks. Both N95 and surgical masks have a stronger association with protection compared with single-layer masks. Eye protection might also add substantial protection. For the general public, evidence shows that physical distancing of more than 1 m is highly effective and that face masks are associated with protection, even in non-health-care settings, with either disposable surgical masks or reusable 12–16-layer cotton ones, although much of this evidence was on mask use within households and among contacts of cases. Eye protection is typically underconsidered and can be effective in community settings. However, no intervention, even when properly used, was associated with complete protection from infection. Other basic measures (eg, hand hygiene) are still needed in addition to physical distancing and use of face masks and eye protection."
Source: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31142-9/fulltext
Distance. Masks. Hygiene. PPE for healthcare workers. Face coverings for everyone. And if you're going into a known, high-risk environment, eye protection.
--
Additional commentary in the Lancet on masks. "For health-care workers on COVID-19 wards, a respirator should be the minimum standard of care. This study by Chu and colleagues should prompt a review of all guidelines that recommend a medical mask for health workers caring for COVID-19 patients. Although medical masks do protect, the occupational health and safety of health workers should be the highest priority and the precautionary principle should be applied. Chu and colleagues also report that respirators and multilayer masks are more protective than are single layer masks. This finding is vital to inform the proliferation of home-made cloth mask designs, many of which are single-layered. A well designed cloth mask should have water-resistant fabric, multiple layers, and good facial fit.
This study supports universal face mask use, because masks were equally effective in both health-care and community settings when adjusted for type of mask use. Growing evidence for presymptomatic and asymptomatic transmission of SARS-CoV-2 further supports universal face mask use and distancing. In regions with a high incidence of COVID-19, universal face mask use combined with physical distancing could reduce the rate of infection (flatten the curve), even with modestly effective masks. Universal face mask use might enable safe lifting of restrictions in communities seeking to resume normal activities and could protect people in crowded public settings and within households."
Source: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31183-1/fulltext
This is important. Saved the best for last, as it were. This is the first mention I've seen of face coverings and distancing being enough to potentially allow for re-opening from a trustworthy, clinical source. If you could have most of life back from before March 2020 (with obvious exceptions like environments where wearing a mask is counterintuitive to the function of the environment, like eating and drinking), but it required a mask at all times, properly used, no exceptions, would you? I would. And I'd gladly help any proprietor nicely escort out anyone who refused compliance. Masks required for every person in every workplace as part of your job unless you literally work alone - if that was the pathway towards resuming economic activity, of restoring lives and livelihoods alike, would you take it?
--
A reminder of the simple daily habits we should all be taking.
1. Wash/sanitize your hands every time you are in or out of your home for any reason. Consider also spraying the bottoms of your shoes with a general disinfectant (alcohol/bleach/peroxide) when you return home. Remember that cleaners are never to be ingested.
2. Wear gloves and a mask when out of your home. Consider wearing a face shield.
3. Stay home as much as possible. Minimize your contact with others and maintain physical distance of at LEAST 6 feet / 2 meters. Avoid indoor places as much as you can.
4. Get your personal finances in order now. Cut all unnecessary costs.
5. Donate any PPE you can. https://getusppe.org/give/
--
Common misinformation debunked!
There is no genomic evidence at all that COVID-19 arrived before 2020 in the United States and therefore no hidden herd immunity:
Source:
There is no evidence SARS-CoV-2 was engineered, nor that it escaped a lab somewhere.
Source: https://www.washingtonpost.com/world/2020/01/29/experts-debunk-fringe-theory-linking-chinas-coronavirus-weapons-research/
Source: https://www.nature.com/articles/s41591-020-0820-9
Source: https://www.nationalgeographic.com/science/2020/05/anthony-fauci-no-scientific-evidence-the-coronavirus-was-made-in-a-chinese-lab-cvd/
There is no evidence a flu shot increases your COVID-19 risk.
Source: https://www.factcheck.org/2020/04/no-evidence-that-flu-shot-increases-risk-of-covid-19/
Source: https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa626/5842161
--
A common request I'm asked is who I follow. Here's a public Twitter list of many of the sources I read.
https://twitter.com/i/lists/1260956929205112834
This list is biased by design. It is limited to authors who predominantly post in the English language. It is heavily biased towards individual researchers and away from institutions. It is biased towards those who publish or share research, data, papers, etc. I have made an attempt to follow researchers from different countries, and also to make the list reasonably gender balanced, because multiple, diverse perspectives on research data are essential.